USAID. MISSION TO KENYA
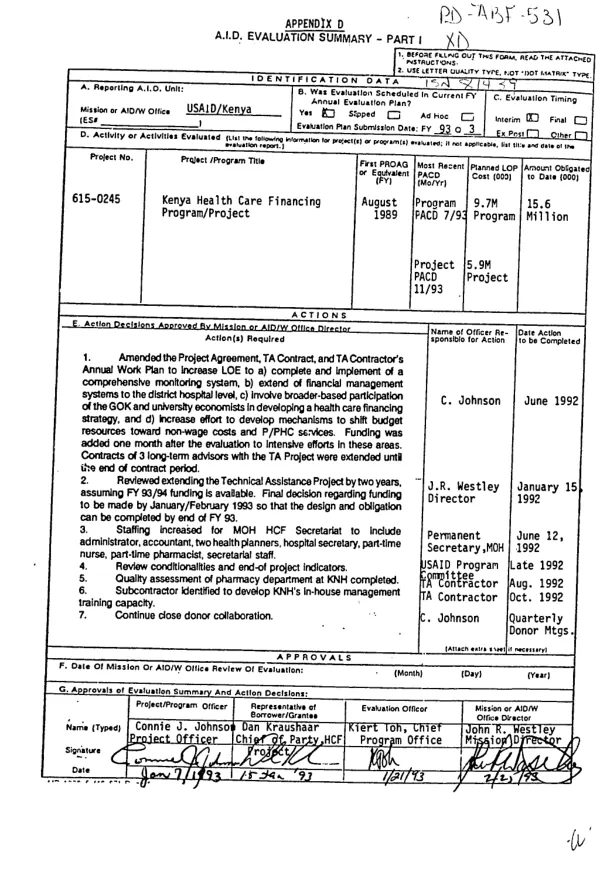
Kenya health care financing program/project
Summarizes attached interim evaluation (XD-ABF-531-A) of a program to increase financial resources for health care, particularly preventive and primary health care, in Kenya.
1993
Sign in to readA free account is required to download.
Abstract
Evaluation covers the period 8/89-5/92. The program has placed Kenya in the forefront of health care finance reform in sub-Saharan Africa and is an excellent example of how nonproject assistance can encourage collaborative efforts in policy reform. All three implementing agencies -- the Ministry of Health (MOH), Kenyatta National Hospital (KNH), and the National Hospital Insurance Fund (NHIF) -- have strengthened their financial management and cost recovery capacities. The cost-sharing system being implemented by the MOH at seven provincial general hospitals shows potential for generating substantial revenues while ensuring that no one is denied care. Of the revenues generated, 75% are used by the collecting facility; this represents 30-80% of facility non-wage operating costs. In addition, the MOH"s Health Care Finance (HCF) Secretariat has developed methods for tracking shifts in resource allocation toward non-wage recurrent costs both in general and with specific regard for preventive and primary health care, and it is initiating an exercise to develop a 5-10 year health care financing policy. The main problems for the MOH have been: (1) it has not developed a system to monitor and evaluate cost-sharing impacts, and (2) the HCF Secretariat is understaffed and has no MOH budget support for operating costs. KNH is utilizing fee collection and accounting systems to support cost-sharing, resulting in revenues that are substantial, though not yet reaching targets. However, KNH (like the MOH) has not yet developed a monitoring and evaluation system for cost-sharing, and has completed only two of six planned quality assessments. Because KNH remains under the MOH"s financial control, it has had problems obtaining funds reserved for it under the Treasury"s allocation; this has placed a great deal of pressure on cost-sharing revenues. The NHIF has developed and implemented a progressive premium structure; reimbursement rates have increased dramatically, resulting in increased revenues at public and private hospital facilities. Contribution and reimbursement rate changes have allowed the group to accumulate a cash surplus which exceeds the levels of reserves normally held by insurance organizations. Unfortunately, the development of new benefits has been deterred by a lack of databases needed for actuarial analysis. Although TA has helped the NHIF refine its claims database, lack of an in-house computing capacity has slowed the process. The following lessons have been learned. (1) The time and effort spent developing a solid analytic base and data on baseline indicators were a good investment. (2) Consensus-building among stakeholders (including public and private organizations and donor agencies) is essential to success. (3) Although extensive plans preceded most of the reforms in this program, problems that threatened program credibility and viability arose in instances where officials took quick action, before implementation plans and without adequate public explanation. (4) A long-term planning perspective (15 years) for phase-in of reforms greatly enhances program viability and permits needed flexibility of policymakers and political leaders. (5) A strong USAID Mission staff role, as well as TA under a project mechanism, are key to achieving the goals of policy reform and nonproject assistance.