USAID DEC
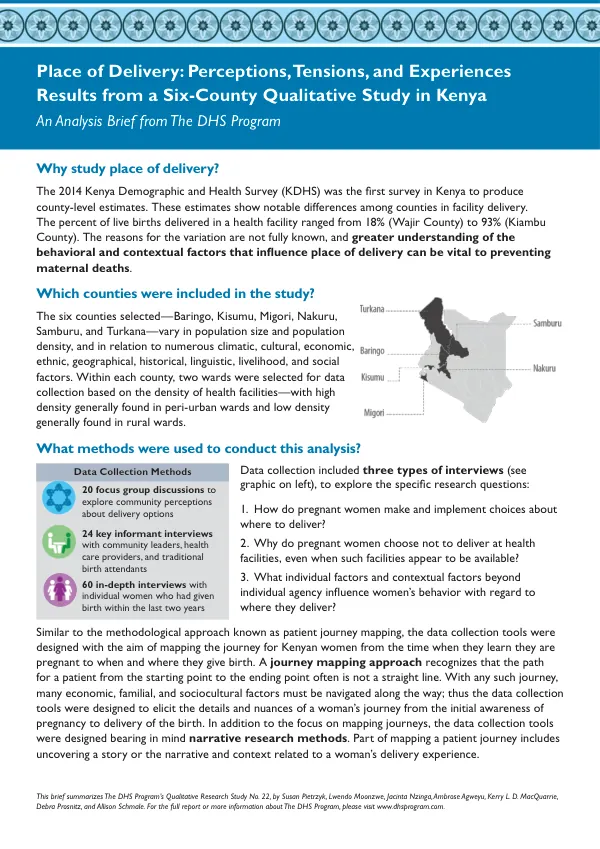
Place of Delivery: Perceptions, Tensions, and Experiences Results from a Six-County Qualitative Study in Kenya
Sign inUSAID DEC
Place of Delivery: Perceptions, Tensions, and Experiences Results from a Six-County Qualitative Study in Kenya
The pregnancy-to-delivery continuum in Kenya is a complex and dynamic process influenced by various individual and collective factors.
2019 · 2 pages
Sign in to readA free account is required to download.
Abstract
The six-county qualitative study conducted in Kenya aimed to explore the behavioral and contextual factors that influence place of delivery. The study selected Baringo, Kisumu, Migori, Nakuru, Samburu, and Turkana counties, which vary in population size, population density, and other factors. Data collection for the study involved three types of interviews: focus group discussions, key informant interviews, and in-depth interviews with individual women who had given birth within the last two years. A total of 20 focus group discussions, 24 key informant interviews, and 60 in-depth interviews were conducted. The data collection tools were designed to map the journey of Kenyan women from the time they learn they are pregnant to when and where they give birth, taking into account the complexities of their experiences. The study's conclusions highlight the importance of contextual factors and decision-making in place of delivery. The pregnancy-to-delivery continuum is characterized by an ever-shifting terrain, influenced by individual and collective beliefs, perceptions, tensions, and experiences. The study found that favorable views about seeking health services at health facilities coexist with interest in traditional approaches, such as the use of herbs. Women often hold traditional birth attendants (TBAs) in high esteem and turn to them when skilled birth attendants (SBAs) are not accessible. The study also identified concerns about inconsistent respectful maternal care at health facilities and variable support from male partners, which can shape decisions about place of delivery. Women sometimes feel insecure and have fears regarding facility delivery and home delivery. The study recommends improving the quality of and accessibility to health care while finding ways for women and their partners to adopt a more health facility-centered approach to maternal care. Key recommendations emerging from the study include continued and coordinated training for health facility staff regarding respectful maternal care, establishing and acting on strategies to overcome transportation challenges and financial burdens, and maintaining balanced and inclusive strategies for promoting health facility delivery. The study also highlights the importance of recognizing cultural beliefs and practices in promoting health facility delivery. The study's findings also shed light on the complexities of perceptions about health care, tensions during pregnancy, experiences during pregnancy, women's narratives of delivery, and male perspectives. Women sometimes view health facility delivery as a means to avoid food-related customs, and TBAs and SBAs may give women different assessments and information about options. Maternity wards often have limited beds for women in labor or ready to deliver, and HIV testing can be both a barrier to and a motivator for facility delivery. The study's conclusions emphasize the need for a more nuanced understanding of the pregnancy-to-delivery continuum in Kenya. By recognizing the complexities of individual and collective factors, policymakers and healthcare providers can develop more effective strategies to improve maternal health outcomes and promote health facility delivery.
Related documents