USAID DEC
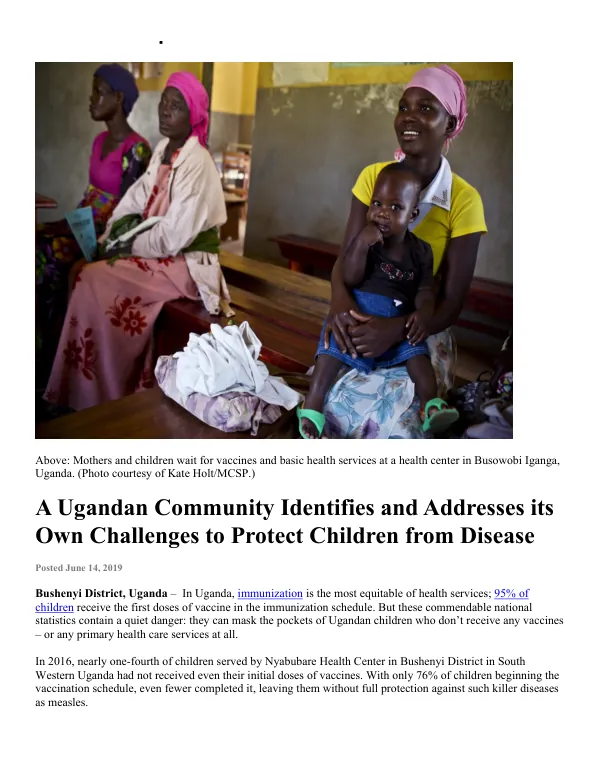
A Ugandan Community Identifies and Addresses its Own Challenges to Protect Children from Disease
Sign inJOHN SNOW INTERNATIONAL
A Ugandan Community Identifies and Addresses its Own Challenges to Protect Children from Disease
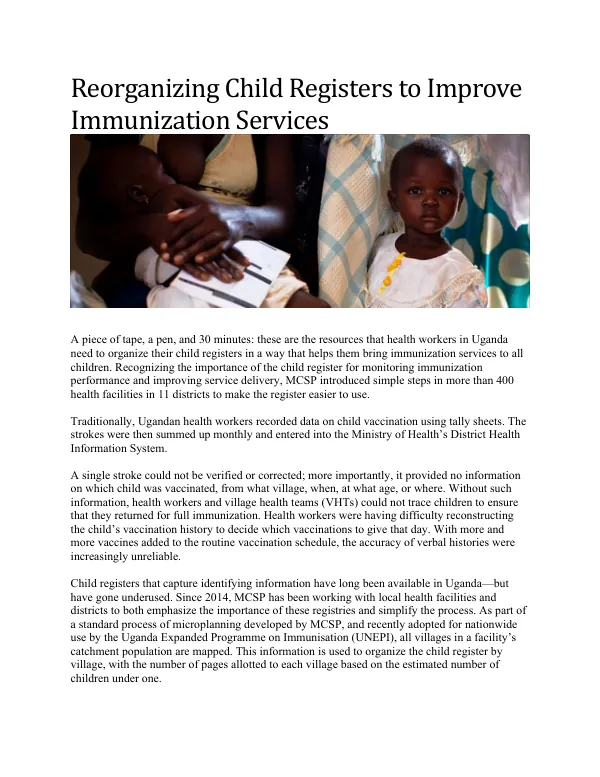
In Uganda, immunization is the most equitable of health services, with 95% of children receiving the first doses of vaccine in the immunization schedule.
2019 · 5 pages
Sign in to readA free account is required to download.
Abstract
However, these commendable national statistics contain a quiet danger: they can mask the pockets of Ugandan children who don't receive any vaccines – or any primary health care services at all. In 2016, nearly one-fourth of children served by Nyabubare Health Center in Bushenyi District in South Western Uganda had not received even their initial doses of vaccines. With only 76% of children beginning the vaccination schedule, even fewer completed it, leaving them without full protection against such killer diseases as measles. MCSP began providing technical support to Bushenyi District in 2016, strengthening the skills of Nyabubare Health Center staff to diagnose their own operational problems and craft locally appropriate solutions. Key to this work was the recognition that both health personnel and community members must work in tandem to uncover the root causes of problems – and overcome them. MCSP and the health center staff worked together to identify the names, locations, and family information of the 400+ children served by the facility, and captured the data in a user-friendly map. By establishing an immunization-focused Quality Work Improvement Team (QWIT) – consisting of both health workers and village health team (VHT) members – they identified the root causes for the low levels of immunization. On the health system side, health workers realized that they were not aware of all the children they were supposed to vaccinate. They had also been reluctant to conduct immunization outreach sessions at sites that were convenient to the community. For their part, VHTs had not known the actions they needed to take to improve immunization. With MCSP support, they learned how to register all children who needed to start the vaccination schedule, and to encourage those who had discontinued the schedule to complete it. The QWIT relocated outreach sites to locations that were more accessible to underserved populations, assigned health workers clear responsibility for immunization activities in certain groups of communities, and assigned VHTs to visit particular homes in their villages and encourage complete vaccination. The collaboration between health staff and VHTs extended beyond health services to include engagement of religious leaders. During church services, these influential leaders began to stress the benefits of complete immunization for their entire congregation. Their role in advocating that all parents get their children fully immunized was key to increasing community demand for vaccination. As a result of this partnership, the number of children who started the vaccination schedule increased by 26% within just one year, from 76% to 91% of all children. Nyabubare Health Center now surpasses the government's target by drawing on its own financial resources and soliciting increased community commitment to protect its children from vaccine-preventable diseases.
Related documents