USAID DEC
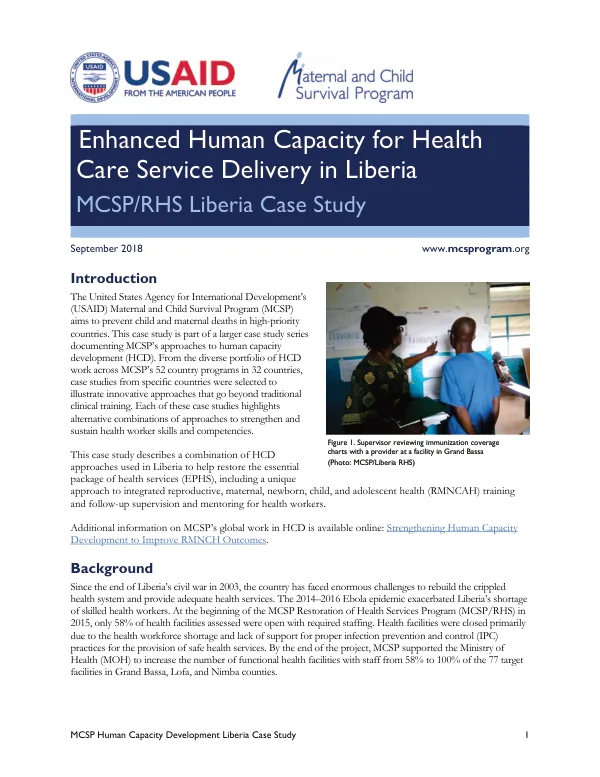
Enhanced Human Capacity for Health Care Service Delivery in Liberia, MCSP/RHS Liberia Case Study
Sign inJHPIEGO
Enhanced Human Capacity for Health Care Service Delivery in Liberia, MCSP/RHS Liberia Case Study
The MCSP Human Capacity Development Liberia Case Study is part of a larger case study series documenting MCSP's approaches to human capacity development (HCD).
2018 · 9 pages
Sign in to readA free account is required to download.
Abstract
The case study describes a combination of HCD approaches used in Liberia to help restore the essential package of health services (EPHS), including a unique approach to integrated reproductive, maternal, newborn, child, and adolescent health (RMNCAH) training and follow-up supervision and mentoring for health workers. Since the end of Liberia's civil war in 2003, the country has faced enormous challenges to rebuild the crippled health system and provide adequate health services. The 2014-2016 Ebola epidemic exacerbated Liberia's shortage of skilled health workers. At the beginning of the MCSP Restoration of Health Services Program (MCSP/RHS) in 2015, only 58% of health facilities assessed were open with required staffing. Health facilities were closed primarily due to the health workforce shortage and lack of support for proper infection prevention and control (IPC) practices for the provision of safe health services. MCSP provided comprehensive support that included capacity building as well as payment of salaries for health facility staff, equipment distribution, and infrastructure upgrades to restore service delivery and improve quality of care in target health facilities. The MCSP Liberia/RHS HCD approach included a combination of specific and integrated skills-based in-service trainings, followed by integrated quality improvement processes such as strengthened supportive supervision and workplace, individual, and team-based mentoring. Integrated in-service training was conducted for health facility staff to ensure that they have the skills and knowledge to provide the MOH's EPHS. The training began with a training of trainers with participants from the three MCSP-supported counties and included officers from the MOH county and district health teams. The training was designed in two four-day sessions using a hands-on, competency-based approach. Both sessions included short segments focused on the different technical areas to troubleshoot the commonly-identified skill and knowledge gaps among providers. Follow-up monthly and quarterly supportive supervision and mentoring were implemented to review and strengthen the national supportive supervision system, including its processes and tools. MCSP worked closely with the MOH to review and strengthen the national supportive supervision system, including its processes and tools. MCSP trained CHT and DHT staff on supervision, coaching, and team-based mentoring skills so that they can provide onsite, team-based and individual mentoring and coaching during supportive supervision visits. Each facility supportive supervision visit lasted one day, beginning with an entry meeting with facility management to review previous action items and ending with a feedback meeting with facility staff. During the visits, supervisors observed the care being provided (if there were no cases during the visit they used simulation cases) and addressed issues on the spot, such as incorrect handwashing, improper partograph plotting, and essential newborn care. Along with the OIC, supervisors reviewed data quality and facility performance against key indicators and targets. The supportive supervision summary tool was developed and implemented to show the status of all action items identified during each visit with copies of summaries kept at health facility and county levels. MCSP county-based staff used CommCare application software to collect and analyze IPC and family planning (FP)-immunization integration data from monthly supportive supervision visits in real time. Collecting data this way made it possible to use the data to inform the focus of supportive supervision visits and to target team-based mentoring and coaching provided during subsequent visits.