USAID DEC
Maternal Health Indicators in High-Priority Counties of Kenya: Levels and Inequities
Sign inUSAID DEC
Maternal Health Indicators in High-Priority Counties of Kenya: Levels and Inequities
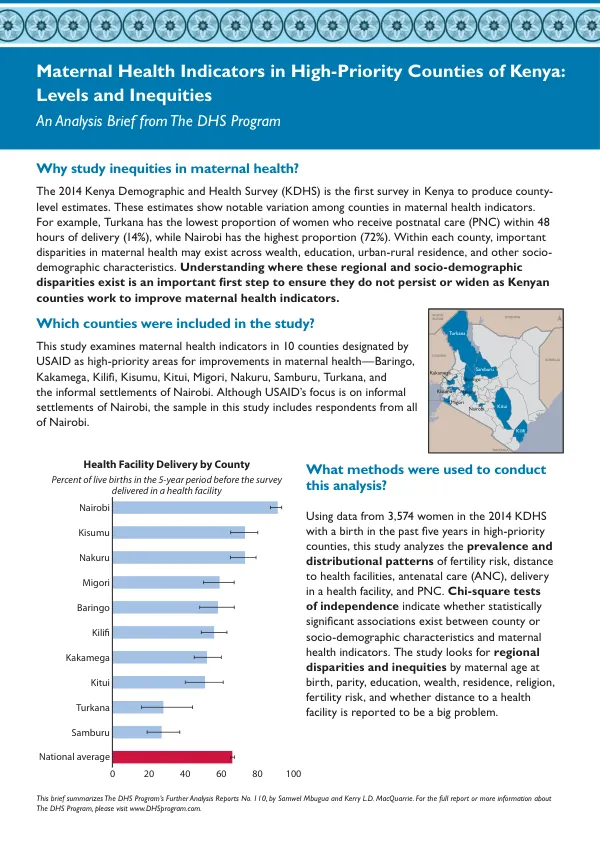
Maternal Health Indicators in High-Priority Counties of Kenya: Levels and Inequities The 2014 Kenya Demographic and Health Survey (KDHS) produced county-level estimates of maternal health indicators, revealing notable variation among counties.
2019 · 2 pages
Sign in to readA free account is required to download.
Abstract
For example, Turkana has the lowest proportion of women who receive postnatal care (PNC) within 48 hours of delivery (14%), while Nairobi has the highest proportion (72%). Understanding regional and socio-demographic disparities in maternal health is crucial to ensure they do not persist or widen as Kenyan counties work to improve maternal health indicators. This study examines maternal health indicators in 10 counties designated by USAID as high-priority areas for improvements in maternal health: Baringo, Kakamega, Kilifi, Kisumu, Kitui, Migori, Nakuru, Samburu, Turkana, and the informal settlements of Nairobi. The analysis uses data from 3,574 women in the 2014 KDHS with a birth in the past five years in high-priority counties. Chi-square tests of independence indicate statistically significant associations between county or socio-demographic characteristics and maternal health indicators. Regional disparities in maternal health indicators are substantial and significant across counties. High-priority counties, other than Nairobi, consistently show disadvantage compared to Kenya as a whole in most maternal health indicators. The study finds a higher number of inequities in the distribution of delivery care and a lower number of inequities in antenatal care (ANC). Inequities are also observed in fertility risk and PNC. The most common disparities at the county level are by women's education, wealth, and urban-rural residence. Turkana shows fewer disparities in maternal health indicators compared to Kilifi, Kisumu, and Kitui. Adequate ANC is defined as four or more ANC visits and the first visit within the first three months of pregnancy. Significant inequities in adequate ANC use by education are found in 6 of the 10 study counties. Disparities in facility delivery by residence are statistically significant in all nine counties where they could be measured, except Turkana. Disparities in PNC within 48 hours of delivery by wealth tercile are found in just four counties but are quite sizable where they exist. County-specific data are necessary for Kenya to achieve equitable provision of healthcare as promoted in the Kenya Health Policy 2012-2030 and Sustainable Development Goals. This study reveals substantial and significant regional variation in all maternal health indicators across counties. The comparison of high-priority counties with national figures suggests that USAID is appropriately focusing its efforts on areas most in need of better maternal health care. As Kenya's county health authorities partner with the national government to improve service delivery under the devolved responsibility for healthcare, all should be aware of the socio-demographic disparities that exist in maternal health within the respective counties. Counties that face numerous inequities could achieve gains in antenatal, delivery, and postnatal care outcomes by focusing efforts on closing disparities. Meanwhile, counties with fewer disparities might want to be mindful that the gaps do not widen as they pursue improvements in maternal health indicators.
Related documents