USAID DEC
2016 WHO Antenatal Care Guidelines: Malaria in Pregnancy Frequently Asked Questions (FAQ)
Sign inUSAID'S MATERNAL AND CHILD SURVIVAL PROGRAM/JOHN SNOW, INC.
2016 WHO Antenatal Care Guidelines: Malaria in Pregnancy Frequently Asked Questions (FAQ)
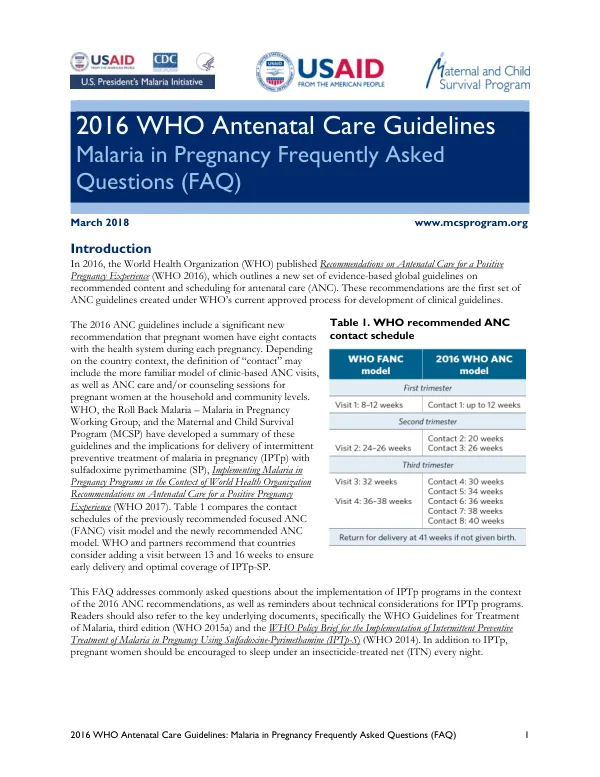
The World Health Organization (WHO) published Recommendations on Antenatal Care for a Positive Pregnancy Experience in 2016, which outlines a new set of evidence-based global guidelines on recommended content and scheduling for antenatal care (ANC).
2018 · 6 pages
Sign in to readA free account is required to download.
Abstract
The guidelines include a significant new recommendation that pregnant women have eight contacts with the health system during each pregnancy. These contacts can include clinic-based ANC visits, as well as ANC care and/or counseling sessions for pregnant women at the household and community levels. The WHO, the Roll Back Malaria – Malaria in Pregnancy Working Group, and the Maternal and Child Survival Program (MCSP) have developed a summary of these guidelines and the implications for delivery of intermittent preventive treatment of malaria in pregnancy (IPTp) with sulfadoxine pyrimethamine (SP). The guidelines recommend that countries consider adding a visit between 13 and 16 weeks to ensure early delivery and optimal coverage of IPTp-SP. The 2016 ANC guidelines emphasize the importance of encouraging pregnant women to sleep under an insecticide-treated net (ITN) every night and to start an IPTp regimen as early as possible in the second trimester. The recommended timing of IPTp is critical, particularly between 13 and 20 weeks when the placenta is forming and parasite densities are highest. To achieve maximum impact, pregnant women should have contact with a health care provider between 13 and 16 weeks gestation to ensure timely access to the first dose of IPTp. The WHO recommends initiating malaria prevention efforts beginning at 13 weeks to achieve major benefit. Pregnant women should receive a second dose of SP one month later to cover this critical period. The example contact schedule in Table 2 accounts for the recommended timing of each dose of IPTp. Any revisions to national ANC guidelines should include provisions to promote early attendance at ANC to ensure that women complete the recommended contacts during the pregnancy. The WHO also emphasizes the importance of counseling pregnant women on the importance of attending all scheduled contacts and helping them plan for scheduled clinic-based ANC. Community health workers should emphasize the importance of attending ANC as early as possible in pregnancy and encourage eight ANC contacts in messaging to community members. Efforts to provide respectful care and reduce disrespect and abuse in health care settings can greatly enhance ANC uptake and attendance. The recommended ANC contact schedule includes the following contacts: * Up to 12 weeks: Register pregnant women, provide ITNs, and counsel on their use. Screen for HIV. Administer 30 to 60 mg of elemental iron and 400 μg (0.4 mg) of folic acid daily. * 13-16 weeks: IPTp-SP dose 1 (additional contact) * 20 weeks: IPTp-SP dose 2 * 26 weeks: IPTp-SP dose 3 * 30 weeks: IPTp-SP dose 4 * 34 weeks: IPTp-SP dose 5 * 36 weeks: No SP (if last dose received <1 month ago) * 38 weeks: IPTp-SP dose 6 (if no dose in last month) * 40 weeks: Pregnant women should receive MiP interventions as appropriate, even when they come at weeks not designated in the contact schedule. Despite the known side effects associated with sulfonamides, SP for IPTp is generally very well tolerated. Mild and transient side effects including nausea, vomiting, weakness, and dizziness have been reported by some women, particularly with the first dose of SP. Studies have demonstrated that side effects tend to decrease with the administration of further doses. Side effects should be discussed openly and managed in the ANC.
Related documents