USAID DEC
Administration of Antenatal Corticosteroids: A Key Intervention to Reduce Mortality and Morbidity Associated with Prematurity
Sign inUNITED NATIONS
Administration of Antenatal Corticosteroids: A Key Intervention to Reduce Mortality and Morbidity Associated with Prematurity
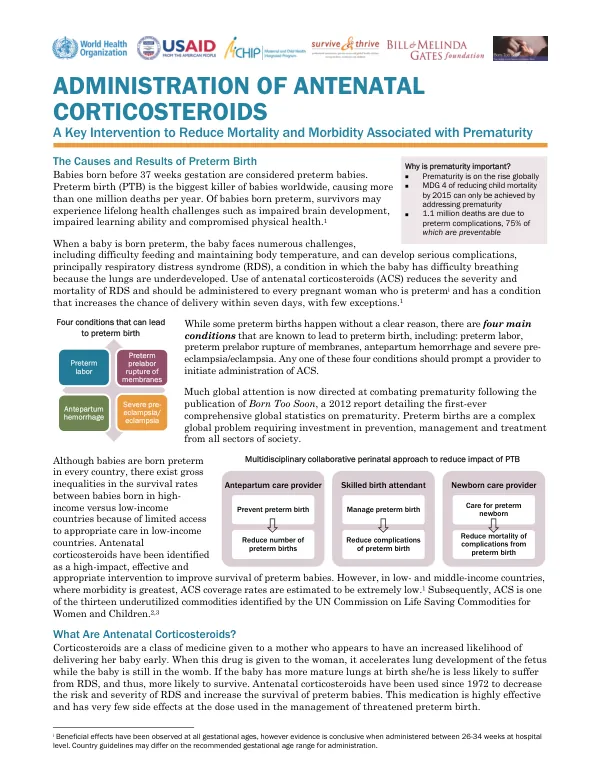
Prematurity is a significant global health issue, with over 1.1 million deaths attributed to preterm complications annually.
2013 · 2 pages
Sign in to readA free account is required to download.
Abstract
Approximately 75% of these deaths are preventable. Premature birth is the leading cause of death among babies worldwide, with more than 1 million deaths occurring each year. Babies born preterm may experience lifelong health challenges, including impaired brain development, impaired learning ability, and compromised physical health. Preterm birth is defined as birth before 37 weeks of gestation. The causes of preterm birth are complex and multifaceted, with four main conditions contributing to the issue: preterm labor, preterm prelabor rupture of membranes, antepartum hemorrhage, and severe pre-eclampsia/eclampsia. These conditions can lead to significant health complications for both the mother and the baby. Administration of antenatal corticosteroids (ACS) has been identified as a key intervention to reduce mortality and morbidity associated with prematurity. ACS work by accelerating fetal lung maturity, reducing the risk of respiratory distress syndrome (RDS), and decreasing the severity of RDS. The medication is highly effective and has very few side effects at the dose used in the management of threatened preterm birth. ACS have been used since 1972 to decrease the risk and severity of RDS and increase the survival of preterm babies. The medication is beneficial at all gestational ages, with conclusive evidence of its effectiveness when administered between 26-34 weeks at hospital level. Country guidelines may differ on the recommended gestational age range for administration. The administration of ACS is typically made by a skilled birth attendant, who can administer the medication to the mother. The medication is given in four doses of dexamethasone 6 mg IM, with the first dose given immediately upon determination that the woman has one of the conditions that increases her likelihood of preterm delivery. The second, third, and fourth doses are given every 12 hours thereafter. Studies have shown that when mothers receive ACS for threatened preterm birth, there is an approximate decrease of 35% in the number of babies who develop respiratory distress syndrome, a 30% decrease in the number of babies needing extra breathing support through assisted ventilation machines, a 45% decrease in babies with cerebral hemorrhage, and a 30% decrease in the number of babies who die. To implement a program for the administration of ACS, health systems need clear national policies and clinical guidelines, inclusion of ACS as a management intervention for threatened preterm birth in the scope of work of each skilled birth attendant qualified to give ACS, consistently available ACS, human and resource capacity to ensure service delivery, and effective monitoring systems to support ACS implementation. ACS are a proven technology that is inexpensive and an appropriate intervention to reduce mortality and morbidity associated with prematurity in low-, middle-, and high-income countries. However, ACS are underutilized in low- and middle-income countries, where morbidity is greatest. Collaborative efforts between policymakers, healthcare professionals, and communities can change this and have a lasting impact on the survival of many more babies worldwide.