USAID DEC
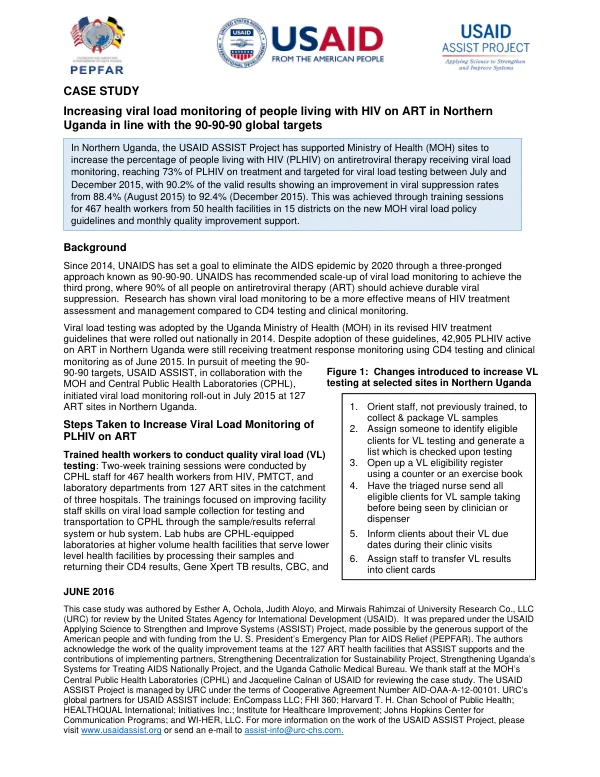
Improving TB Treatment Response Monitoring at Nine TB Diagnostic Treatment Units: Tested Changes and Guidance from Uganda
Sign inENCOMPASS, LLC
Improving TB Treatment Response Monitoring at Nine TB Diagnostic Treatment Units: Tested Changes and Guidance from Uganda
Uganda continues to notify thousands of tuberculosis (TB) cases, with 46,171 TB cases reported in 2014, but these are only half of the estimated TB cases (87,000) according to the Uganda National Population Based Tuberculosis Prevalence Survey 2014-2016.
2018 · 16 pages
Sign in to readA free account is required to download.
Abstract
The annual risk of TB infection (ARI) for Uganda remains high at three percent, with an incidence of TB at 234 per 100,000 population and prevalence of TB at 253 per 100,000 population. The mortality rate from TB (excluding HIV-positive TB patients) in 2014 was estimated at 12 per 100,000 population. Multi-drug resistant TB (MDR-TB) is an emerging problem, with more than 1,040 estimated cases every year, but the actual case finding is only around 200 cases per year. The quality of TB services is low, with several TB diagnostic and treatment units (DTUs) in the hands of lower cadres of health workers. According to the Ministry of Health's (MOH) National Tuberculosis and Leprosy Program (NTLP), all bacteriologically confirmed TB cases should have a sputum microscopy (or culture) performed at the end of the initial phase (two months), at the beginning of fifth month, and the beginning of the sixth month of treatment. This is done for both smear-positive and smear-negative pulmonary TB patients. The importance of sputum follow-up smears is to assess treatment response, assess patients' adherence to medications, to find if bacillary load has reduced, and to identify treatment failures/MDR-TB. USAID, through the Applying Science to Strengthen and Improve Systems (ASSIST) project in Uganda, is working in collaboration with the MOH and implementing partners (IPs) to build the capacity of health workers to be able to screen, diagnose, and manage TB to improve TB care services using the continuous quality improvement (QI) model as well as the collaborative approach. In January 2016 to September 2016, USAID ASSIST together with the MOH and regional IPs provided support to 15 selected health facilities in Eastern, East Central, Central Kampala Capital City Authority (KCCA), and South Western regions. They conducted eight monthly onsite coaching visits, two learning sessions, and one harvest meeting to ensure TB care services improved at all the TB supported facilities for a period of eight months. The baseline assessment conducted in October 2015 at the participating health facilities found that sputum follow-up monitoring was at 55.8% at two months, 34.1% at five months, and 31.5% at 6/8 months of TB treatment. USAID ASSIST engaged the facility-based health workers to into regular review and analysis of performance on sputum follow-up monitoring and identify possible process changes to test and implement. In December 2015, ASSIST provided orientation on the basics of QI to the TB case providers through a training. This was followed with regular (at least monthly) support to the teams through onsite coaching to review performance and for teams to come up with service innovations (changes) which they tested to attain better sputum follow-up monitoring rates. The change package for improving TB treatment response monitoring at nine TB diagnostic treatment units was developed based on the experience gained while working with the 15 selected health facilities. The package includes documentation requirements and tools, results, and a harvest meeting. The intended use of the change package is to provide guidance and support to health facilities in improving TB treatment response monitoring. The package is designed to be used by facility-based health workers to review performance, identify possible process changes, and implement service innovations to attain better sputum follow-up monitoring rates. The recommendations from the change package include regular review and analysis of performance on sputum follow-up monitoring, identification of possible process changes to test and implement, and provision of orientation on the basics of QI to TB case providers. The package also recommends regular onsite coaching to review performance and for teams to come up with service innovations (changes) which they tested to attain better sputum follow-up monitoring rates. The annex to the change package includes rank-ordered changes to improve sputum follow-up at two months, a list of facilitators during the harvest meeting, and participating sites and their QI teams. The change package is intended to be used by health facilities in Uganda to improve TB treatment response monitoring. The package is designed to be used by facility-based health workers to review performance, identify possible process changes, and implement service innovations to attain better sputum follow-up monitoring rates. The recommendations from the change package are based on the experience gained while working with the 15 selected health facilities and are intended to be used by health facilities in Uganda to improve TB treatment response monitoring.