USAID
MOMENTUM Nigeria Country Profile - Immunization
Routine Immunization Transformation and Equity in Nigeria is a critical component of the country's Basic Minimum Package of Health Services.
2021 · 5 pages
Sign in to readA free account is required to download.
Abstract
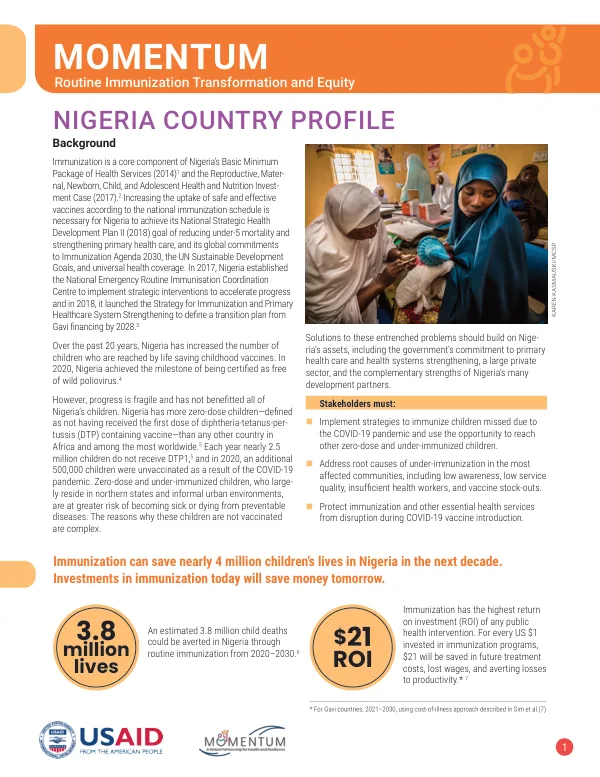
Immunization is essential for achieving Nigeria's National Strategic Health Development Plan II goal of reducing under-5 mortality and strengthening primary health care. The country has made progress in increasing the number of children reached by life-saving childhood vaccines, with Nigeria being certified as free of wild poliovirus in 2020. However, progress is fragile, and Nigeria has more zero-dose children than any other country in Africa and among the most worldwide. Zero-dose children are defined as those not having received the first dose of diphtheria-tetanus-pertussis (DTP) containing vaccine. In 2020, 35% of infants in Nigeria did not receive DTP1. The reasons for this are complex, including low awareness, low service quality, insufficient health workers, and vaccine stock-outs. Stakeholders must implement strategies to immunize children missed due to the COVID-19 pandemic and use the opportunity to reach other zero-dose and under-immunized children. Addressing root causes of under-immunization in the most affected communities is also crucial. Immunization has the highest return on investment (ROI) of any public health intervention. For every US $1 invested in immunization programs, $21 will be saved in future treatment costs, lost wages, and averting losses to productivity. An estimated 3.8 million child deaths could be averted in Nigeria through routine immunization from 2020-2030. Immunization can save nearly 4 million children's lives in Nigeria in the next decade. Investments in immunization today will save money tomorrow. The majority of Nigeria's zero-dose children live in northern states, but even within these states, access and coverage vary widely. Despite higher coverage in southern states, informal settlements near Lagos and other cities harbor many of Nigeria's zero-dose children. Qualitative and survey research from Nigeria suggests that multiple factors can be mitigated with tailored strategies. DTP3 coverage is increasing, but gaps between the poorest and richest persist. Vaccine availability has improved since 2016, but in December 2020, 24% of rural and 40% of urban health facilities were stocked out of pentavalent vaccine. Nigeria relies on development partners for financing immunization, with approximately two-thirds of the immunization budget coming from external sources. Nigeria will transition from Gavi support by 2028 and faces tremendous challenges in financing its immunization program amidst the existing constraints and the emerging economic impacts of the COVID-19 pandemic. There are significant gaps in health worker performance, including a 28.8% provider absenteeism rate and gaps in health worker salary payment. Strengthening investments in integrating immunization with other primary health care services to improve efficiency and reach of services is crucial. To support Nigeria's financing goals, USAID and other partners should consider strengthening investments in integrating immunization with other primary health care services, supporting advocacy to federal and state-level government to increase domestic resources for immunization and primary health care, and participating in annual reviews of the accountability framework for Nigeria's transition. The COVID-19 pandemic disrupted routine immunization and other essential health services, with not all missed children having been reached. The project estimated an additional 500,000 children were missed in 2020, compared to previous years.
Related documents