USAID DEC
Project assistance completion report : the private voluntary organizations for health project (386-0469)
Sign inUSAID. MISSION TO INDIA
Project assistance completion report : the private voluntary organizations for health project (386-0469)
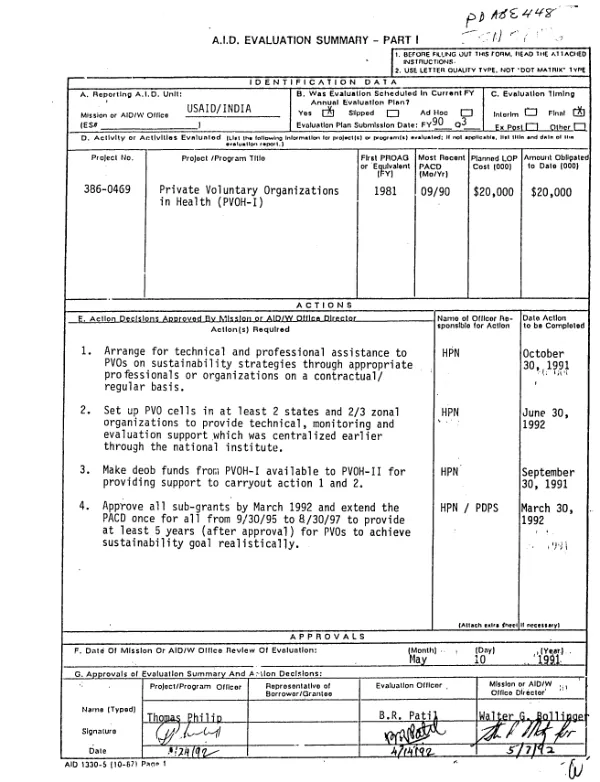
PACR of a project (8/81-9/90) to reduce mortality and fertility among rural and urban poor in India by supporting joint efforts of USAID, the Government of India (GOI) and PVOs involved in health and population.
1970
Sign in to readA free account is required to download.
Abstract
The project was very successful, expanding and improving basic and special preventive health, family planning, and nutrition services for the poor by strengthening the private and voluntary sector. It also fostered cooperation among the GOI, USAID, and PVOs by agreeing on the untapped potential of PVOs and by sharing program costs. The program approved sub-grants to 30 PVOs, affecting 1.5 million individuals in underserved areas. Beyond the quantity of projects, the quality of the services maintained high standards. The voluntary sub-grantees greatly strengthened their capabilities to manage health projects and to deliver a quality package of maternal/child health interventions, including immunization, oral rehydration therapy, health education, family planning, and prenatal care. This was a result of training large numbers of workers, increasing the number of staff members at all levels and expanding operations to cover a significant number of people in underserved and isolated areas. The project also assisted the PVOs in developing better financial systems and upgrading their project monitoring capabilities. Regarding the government sector, the Ministry of Health and Family Welfare (MOHFW) and the National Institute of Health and Family Welfare (NIHFW) developed a much better understanding of PVOs and what they an accomplish in the health field, as well as a sensitivity and capability to work more effectively with them. The NIHFW played a critical role in the success of the project by assuring the technical quality of subprojects and providing appraisal, monitoring and evaluation. The MOHFW"s attitude has changed from one of having to tolerate the voluntary sector to one in which it considers a PVO the best mechanism to reach remote and resistant population pockets with family welfare and health services. The enthusiasm with which the GOI/MOHFW is advocating collaboration with PVOs indicates that the shift is genuine and not superficial. The following lessons were learned. (1) The GOI and PVOs can collaborate effectively, especially using an intermediary technical institution to monitor results and quality control. (2) Comprehensive sustainability planning needs to be incorporated into the initial project design with adequate TA at the project design and appraisal stage. (3) While PVOs had sufficient technical competence in the health and family welfare areas, they could have been more effective if assistance had been provided in accounting procedures and managerial skills. (4) Small grassroots organizations were unable to access grant funds because USAID grants are too large for them to absorb, yet they work in the most needy areas. (5) PVOs are constrained from expanding their services by lack of trained grassroots level workers. (6) Closer involvement between the PVOs and the local state governments should be fostered to change the states" perception that the project was out of their purview and control. (7) An effective way to influence GOI policy is to design and implement an activity with no overt suggestion of policy changes. Although this approach may require considerable time, once the GOI is convinced that the new methods can lead to success, it is often quick to change its policies. In India, USAID is the accepted leader in strengthening the PVO sector. Efforts have been aimed at individual PVOs, while strengthening the sector as a whole has been neglected. It is recommended that future projects focus on the national PVO sector to enhance its ability to function as an effective third alternative to the government and commercial sectors in the field of health services.