WORLD HEALTH ORGANIZATION
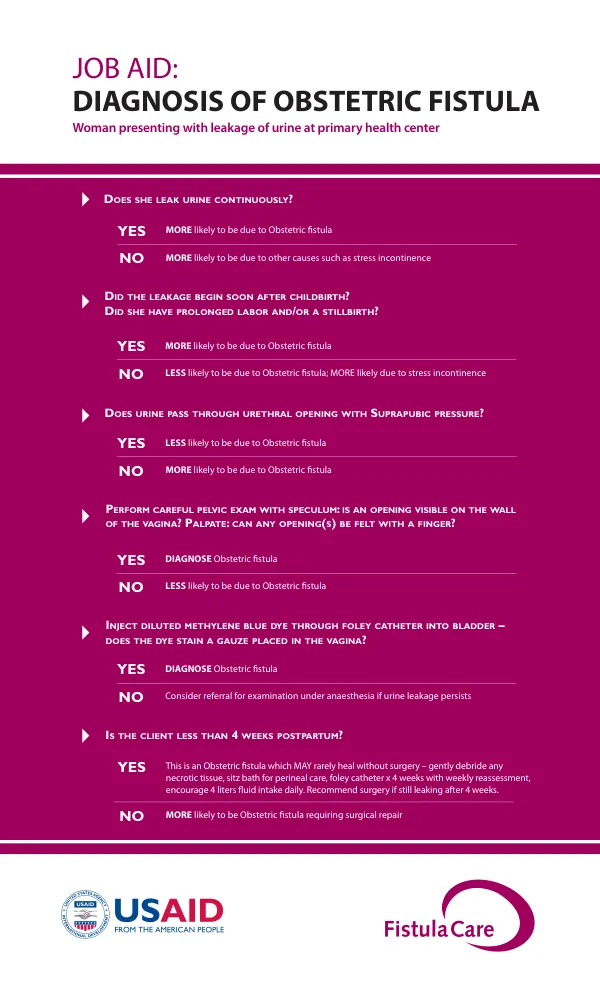
Diagnosis and Treatment of Obstetric Fistula
Obstetric fistula is a condition characterized by an abnormal connection between the bladder and the vagina, resulting in continuous urine leakage.
2 pages
Sign in to readA free account is required to download.
Abstract
The condition is often caused by prolonged labor and obstructed childbirth, which can lead to tissue death and fistula formation. Diagnosis of obstetric fistula typically involves a combination of clinical evaluation and laboratory tests. A careful pelvic exam with speculum and palpation can help identify the presence of an opening on the wall of the vagina or a palpable fistula. Injecting diluted methylene blue dye through a foley catheter into the bladder and observing the dye's staining of a gauze placed in the vagina can also confirm the presence of a fistula. The management of obstetric fistula involves a multidisciplinary approach, including medical, nutritional, and counseling components. Initial treatment may include debridement of necrotic tissue, sitz baths for perineal care, and a foley catheter for 4 weeks with weekly reassessment. Patients are also encouraged to drink at least 4 liters of fluid per day. Surgery is recommended if urine leakage persists after 4 weeks. Nutritional support is essential for patients with obstetric fistula, and a high-protein diet with iron and folate supplements is recommended. Laboratory screening, including blood type and Hgb, urine microscopy, and stool for parasites, can help identify underlying conditions that may be contributing to the fistula. Preparation for obstetric fistula repair involves a thorough evaluation of the patient's condition. The fistula's size, location, and extent of vaginal scarring are assessed, as well as the presence of any additional complications, such as stool in the vagina or foot drop. If the fistula is simple and does not involve any of these complications, the patient can be prepared for repair. However, if the fistula is complex or involves additional complications, the patient may require referral to a specialist for more extensive preparation and surgery. The World Health Organization has developed guiding principles for the clinical management and program development of obstetric fistula. These principles emphasize the importance of early antenatal care, skilled attendance, and the potential benefits of cesarean delivery for future pregnancies. Counseling is also an essential component of obstetric fistula management, and patients are advised to refrain from penetrative sexual relations for 3 months after surgery and to expect some degree of incontinence even after repair. Several studies have investigated the risk factors that predict failure after vaginal repair of obstetric vesicovaginal fistulae. These studies have identified factors such as the size and location of the fistula, the presence of vaginal scarring, and the patient's overall health status as predictors of successful repair.
Related documents