ABT ASSOCIATES
Health Financing Profile: Côte d'Ivoire
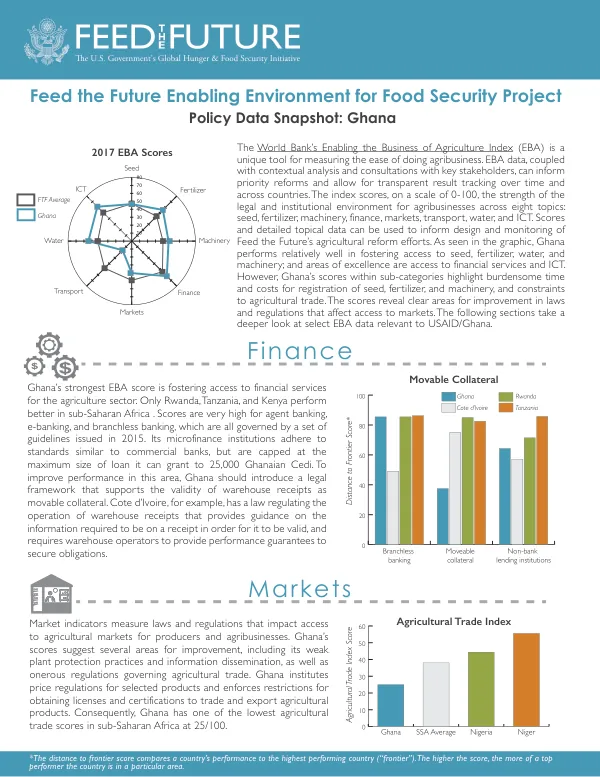
Côte d'Ivoire's total population is approximately 22.6 million people, with a total fertility rate of 4.8 births per woman.
2016 · 2 pages
Sign in to readA free account is required to download.
Abstract
The country's gross national income per capita is $3,130 in purchasing power parity (PPP) terms, as of 2014. Health care expenditure indicators show that the total expenditure on health as a percentage of GDP is 5.7%, which is lower than the global average of 9.2% and the average for low-income countries of 5%. The level of expenditures on health care in Côte d'Ivoire is characterized by a general government expenditure on health as a percentage of total government expenditure of 8.5%, which is below the target set by the Abuja Declaration of 15%. Per capita total expenditure on health is $172 in PPP terms, while per capita government expenditure on health is $57 in PPP terms. The majority of private expenditure on health is out-of-pocket spending, accounting for 76.5% of private expenditure. Sources of funds for health care in Côte d'Ivoire include general government expenditure on health, private expenditure on health, and external resources for health. The government expenditure on health accounts for 33.1% of total expenditure on health, while private expenditure accounts for 66.9%. External resources for health account for 7.7% of total expenditure on health. The country's health care system is dominated by the public sector, with three levels of health facilities: primary, secondary, and tertiary. The primary level consists of sanitary institutions of first contact, including health centers, specialized health centers, and clinics. The secondary level includes health facilities used for first referrals, such as general, regional, and specialized hospitals. The tertiary level includes health facilities used for second referrals, such as teaching hospitals and specialized national institutes. The private sector also plays a significant role in the provision of health care services, with non-profit, for-profit, and traditional medicine providers contributing to the country's health care supply. Private for-profit health care facilities account for over 25% of the country's health care supply. In 2012, the National Health Development Plan (PNDS) was launched, setting the goal of creating a high-quality health system to guarantee the highest possible level of health for all citizens. The PNDS prioritized health financing as a strategic area for improving the health and well-being of the population. The plan aimed to increase health financing through mobilization of internal and external resources, strengthen integration of health financing, allocate resources with priority given to primary health care, and ensure well-managed use of financial resources. In May 2014, the government enacted mandatory health care coverage for all residents of Côte d'Ivoire, establishing the National Health Insurance Fund (NHIF) as a single national fund to consolidate, manage, and regulate existing health financing schemes. The NHIF offers two schemes: a contributory Basic General Scheme (RGB) and a non-contributory Medical Assistance Scheme (RAM) for low-income persons or those living in extreme poverty. The RGB is a contributory scheme based on the principle of third-party payment and co-payment, while the RAM is a non-contributory scheme based on the principle of national solidarity. The NHIS mandates coverage for all citizens, with the first stage rollout prioritizing private and public sector employees, retired persons, and producers of rubber and palm oil. The benefits package provides basic coverage of health services, including consultations, medications, surgery, exams, laboratory tests, and hospitalizations. Achieving universal health coverage (UHC) requires equitable access to health services and financial risk protection. Currently, less than 10% of Côte d'Ivoire's population has adequate health coverage, with 51% of total health spending paid out-of-pocket by households. The government spends a significantly larger share of funds on tertiary care than on secondary or primary care, which is unfavorable to the poor who are more likely to use primary care. Equity in financing and utilization is a significant challenge in Côte d'Ivoire, with 60% of women in the poorest quintile mentioning distance to health services as a major barrier to maternity care, compared to 25% for women in the wealthiest quintile. The government will need to expedite the rollout of the NHIS, identify those most vulnerable, and advocate for increased resource allocation from internal and external partners to increase health care coverage for the population.
Related documents