USAID
Improved Labor Care to Reduce Intrapartum-Related Newborn Deaths
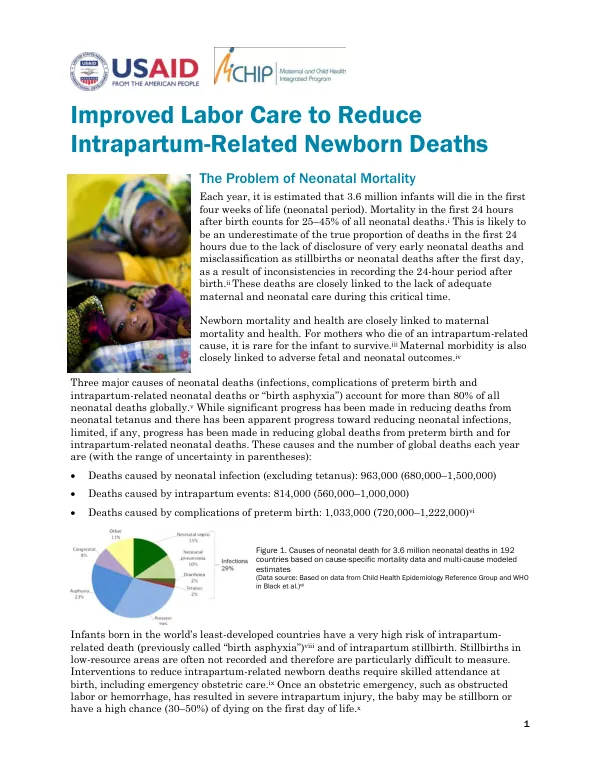
Improved Labor Care to Reduce Intrapartum-Related Newborn Deaths Each year, approximately 3.6 million infants die in the first four weeks of life, with 25-45% of these deaths occurring in the first 24 hours after birth.
2011 · 4 pages
Sign in to readA free account is required to download.
Abstract
This mortality rate is likely underestimated due to inconsistencies in recording the 24-hour period after birth. Newborn mortality is closely linked to maternal mortality, with mothers who die of intrapartum-related causes rarely having their infants survive. Three major causes of neonatal deaths account for more than 80% of all neonatal deaths globally: infections, complications of preterm birth, and intrapartum-related neonatal deaths. While significant progress has been made in reducing deaths from neonatal tetanus and infections, limited progress has been made in reducing global deaths from preterm birth and intrapartum-related neonatal deaths. The causes of neonatal death are estimated to be: * Neonatal infections (excluding tetanus): 964,000 (680,000-1,500,000) * Intrapartum events: 814,000 (560,000-1,000,000) * Complications of preterm birth: 1,033,000 (720,000-1,222,000) Infants born in the world's least-developed countries have a high risk of intrapartum-related death and intrapartum stillbirth. Interventions to reduce intrapartum-related newborn deaths require skilled attendance at birth, including emergency obstetric care. Efforts to improve labor care and reduce newborn deaths focus on prevention of infection, birth trauma, and asphyxia. The prevention of intrapartum-related newborn deaths can be influenced by the care a woman receives during labor. Vigilance during labor is essential, as monitoring the mother and baby can detect complications early and prevent morbidity and mortality. Monitoring the fetal heart rate every 30 minutes during the active phase of labor and every five minutes during the expulsive stage of labor is crucial. If monitoring reveals fetal heart rate abnormalities, appropriate interventions should be taken, such as position changes, oxygen administration, maternal rest, or assisted vaginal delivery or cesarean section. The partograph is a decision-making tool that records the condition of the mother and baby, as well as the progress of labor. Its use has been shown to reduce prolonged labor, the proportion of labors requiring augmentation, and emergency cesarean sections, as well as intrapartum stillbirths and early newborn deaths. Clinical practices to be promoted to reduce intrapartum-related newborn deaths include: * Skilled attendance at every birth * Use of the partograph * Companionship during labor and birth * Rest between pushing in the second stage of labor * Food and drink during labor * Appropriate management of pre-eclampsia * Appropriate use of cesarean section Clinical practices to be avoided to reduce intrapartum-related newborn deaths include: * Restriction of movement during labor * Supine position during labor and birth * Uninterrupted pushing during the second stage of labor * Uncontrolled use of oxytocin In addition to using the partograph, augmentation of labor should be carried out only for medical reasons, and oxytocin should be administered according to protocols in the World Health Organization's manual. Oxytocin should never be given in an uncontrolled or unmonitored manner. Supportive management during the first stage of labor can improve birth outcomes for both the mother and baby. Providing emotional support, using nonpharmacologic pain relief measures, and ensuring adequate hydration and nutrition can reduce the need for operative deliveries and pharmacologic analgesia. The management of pre-eclampsia/eclampsia is crucial, as these diseases can impact newborns. Recognizing and managing severe pre-eclampsia may necessitate preterm delivery, which can result in neonatal complications. Skilled management of the second stage of labor is essential, as it begins when the cervix is fully dilated. The woman should push only with contractions and rest in between them, allowing deep breathing to re-oxygenate the uterus and placenta.
Related documents