WORLD HEALTH ORGANIZATION
Maternal Mortality and HIV: An Overview
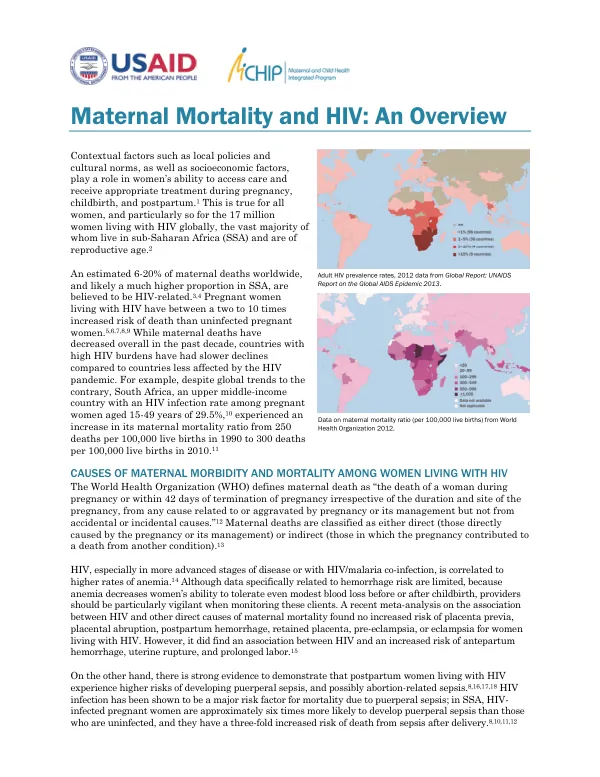
Maternal Mortality and HIV: An Overview The risk of maternal mortality is significantly higher for women living with HIV, particularly in sub-Saharan Africa.
2013 · 4 pages
Sign in to readA free account is required to download.
Abstract
An estimated 6-20% of maternal deaths worldwide are believed to be HIV-related, with a much higher proportion in sub-Saharan Africa. Pregnant women living with HIV have a two to 10 times increased risk of death compared to uninfected pregnant women. The World Health Organization defines maternal death as the death of a woman during pregnancy or within 42 days of termination of pregnancy, from any cause related to or aggravated by pregnancy or its management. Maternal deaths are classified as either direct or indirect, with HIV being a major risk factor for indirect causes of maternal mortality. HIV, especially in more advanced stages of disease or with HIV/malaria co-infection, is correlated with higher rates of anemia, which can lead to increased risk of maternal mortality. Studies have demonstrated that pregnant women living with HIV experience higher risks of developing puerperal sepsis, and possibly abortion-related sepsis. HIV infection has been shown to be a major risk factor for mortality due to puerperal sepsis, with women living with HIV being approximately six times more likely to develop puerperal sepsis than those who are uninfected. Tuberculosis (TB) is a leading cause of maternal morbidity and mortality in settings with a high HIV burden. Co-infection with TB and HIV raises particular concerns, as HIV increases reactivation of TB and increases TB mortality. Antiretroviral therapy (ART) for pregnant women living with HIV, and proper identification and treatment of TB, can decrease the risk of dying of both HIV and TB. Pregnant women living with HIV may also have other concurrent infections, depending on the local context. Co-infection with malaria is common in areas of high prevalence of both diseases. Women living with HIV have a three-fold higher risk of severe anemia and five-fold higher risk for maternal death due to malaria than their HIV-negative counterparts. The 2013 World Health Organization guidelines recommend that women with CD4 counts of 500 or higher remain on ART through cessation of breastfeeding, and women with CD4 counts below 500 continue ART for life. ART substantially reduces HIV-related maternal mortality, but there is a need for further data on how much maternal mortality could be reduced by increasing the number of women on ART. Women who start on ART during pregnancy should be provided adequate clinical and social support to help them stay on ART to maintain their own health as well as the health of their families. Routine follow-up is important to monitor for potential drug toxicity, and women who initiate ART at very low CD4 counts should be followed closely as they may be at risk for immune reconstitution inflammatory syndrome (IRIS). Globally, there were an estimated 19,000-56,000 maternal deaths attributed to HIV-related causes in 2011. Many of these deaths can be prevented with the implementation of high-quality antenatal, obstetric, and postpartum care, including prompt diagnosis of HIV and associated opportunistic infections, prevention and treatment of common co-infections, and provision of ART. It is essential that women living with HIV have access to early antenatal care, integration of screening, prevention, and treatment of HIV and other infectious diseases into the maternal health care platform, and empowerment of nurses and midwives to prescribe ART. The maternal health and HIV communities must converge to identify gaps in the collective understanding of the intersection of maternal health and HIV infection. This will require a comprehensive approach to addressing the complex issues surrounding maternal mortality and HIV, including the provision of high-quality antenatal, obstetric, and postpartum care, and the integration of HIV services into the maternal health care platform.
Related documents
Documents in this collection
 2019
2019USAID DEC
Designing interoperable health information systems using Enterprise Architecture approach in resource-limited countries: A literature review
Open record 2019
2019USAID DEC