USAID
PROFIL DE FINANCEMENT DE LA SANTÉ: ÉTHIOPIE
The Ethiopian health financing profile is characterized by a significant public sector presence in the healthcare sector.
2016 · 2 pages
Sign in to readA free account is required to download.
Abstract
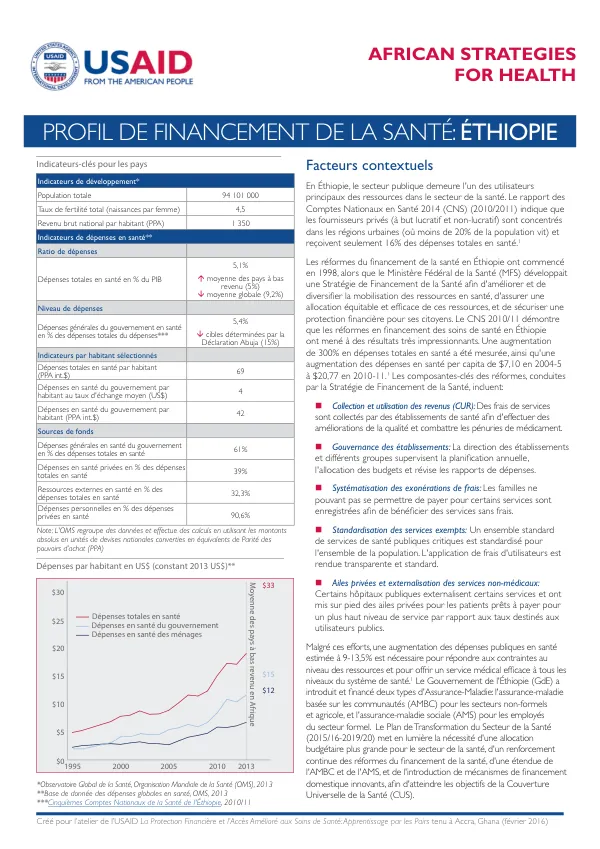
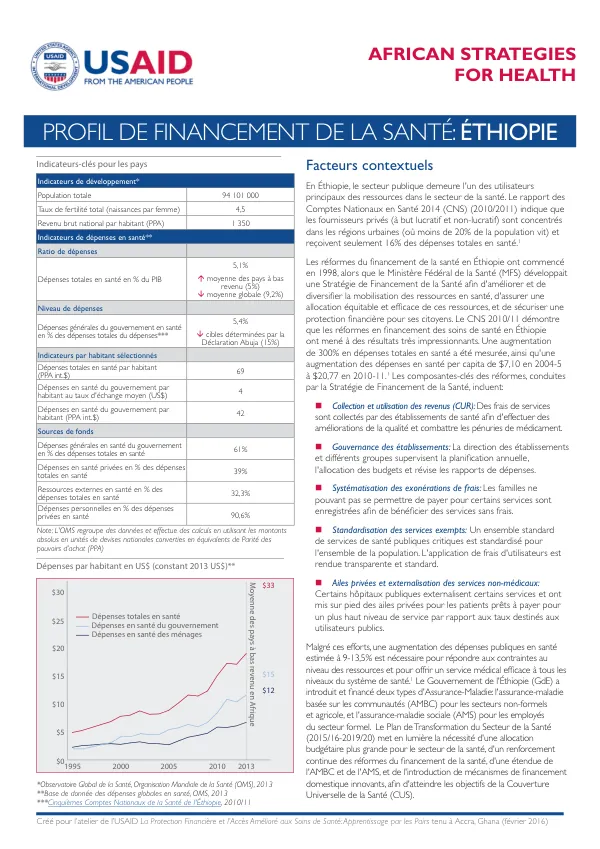
The 2014 National Health Accounts (NHA) report indicates that public providers are the primary users of resources in the sector, with private providers (for-profit and non-profit) concentrated in urban areas, where less than 20% of the population resides, and receiving only 16% of total health expenditures. The health financing reforms in Ethiopia began in 1998, with the Federal Ministry of Health (FMOH) developing a Health Financing Strategy to improve and diversify the mobilization of health resources, ensure equitable and efficient allocation of these resources, and secure financial protection for citizens. The NHA 2010/11 report demonstrates that the health financing reforms in Ethiopia have led to impressive results, with a 300% increase in total health expenditures and a 60% increase in per capita health expenditures from $7.10 in 2004-5 to $20.77 in 2010-11. The key components of the health financing reforms, conducted by the Health Financing Strategy, include: 1. Revenue collection and utilization: Service fees are collected by health facilities to improve quality and combat shortages of medicines. 2. Governance of health facilities: Facility management and supervisory groups oversee annual planning, budget allocation, and review of expenditure reports. 3. Standardization of exempt services: A standardized set of critical public health services is established for the entire population, with transparent and standardized user fees. 4. Private wings and outsourcing of non-medical services: Some public hospitals outsource certain services and establish private wings for patients willing to pay for a higher level of service compared to public user rates. 5. Community-based health insurance (CBHI) and social health insurance (SHI): The government has introduced and financed two types of health insurance: CBHI for the informal and agricultural sectors, and SHI for formal sector employees. Despite these efforts, an estimated 9-13.5% increase in public health expenditures is necessary to address resource constraints and provide effective healthcare services at all levels of the healthcare system. The Ethiopian government has introduced and financed two types of health insurance: CBHI for the informal and agricultural sectors, and SHI for formal sector employees. The Plan of Transformation of the Health Sector (2015/16-2019/20) highlights the need for a larger budget allocation for the health sector, continued strengthening of health financing reforms, expansion of CBHI and SHI, and introduction of innovative domestic financing mechanisms to achieve the Universal Health Coverage (UHC) goals. The health financing approach in Ethiopia is primarily based on needs (inputs) rather than outcomes (outputs). Harmonization of external donor funding (which represents half of external assistance) and better planning and coordination between regional governments and the FMOH could lead to greater efficiency in resource utilization. The government contributes through general subsidy payments to cover expenses for hospitalized and non-hospitalized patients, surgeries, medicines, and households enrolled. Currently, 6.5 million people are enrolled in the CBHI system, which constitutes 7% of the country's total population (national health insurance coverage was less than 1% two years ago). In comparison, SHI is based on employment and is mandatory for public sector employees before it is extended to private sector employees. The implementation of the program is planned for January 2016. For these two risk-sharing arrangements, the government must prudently calibrate the benefit design, payment mechanisms for providers, and coordinate subsidies within and between programs. The FMOH has established the Ethiopian Health Insurance Agency (EHIA) to jointly manage the CBHI and SHI programs. The EHIA is currently working with development partners to evaluate lessons and contribute to decision-making based on observations regarding payment mechanisms. A significant portion of healthcare services (61%) is reimbursed in the form of government expenditures. However, more than 35% comes from household expenditures. Performance-based contracts are used to improve service offerings, transferring money from buyers (the Ministry of Health, regional health bureaus, and district health offices) to service providers (health facilities) conditionally to predetermined performance targets. Under the CBHI program, providers are reimbursed on a fee-for-service basis. Reimbursements for services provided to CBHI members, combined with revenue collection by health facilities, have increased the availability of resources for healthcare within facilities. Achieving Universal Health Coverage (UHC) UHC can only be achieved if healthcare services and financial protection against risks are equitably distributed. Equitable financial protection means that every person, regardless of income level, has access to healthcare services they need without causing significant financial difficulties. Financial Protection Estimates of the financial burden in the form of household expenditures range from 1.07% to 4% of income. To improve financial protection, the government has established fee exemption programs, CBHI pilot programs, and a legal context for health insurance in the formal sector. Services offered by facilities do not require copayments for individuals enrolled in pilot programs. The Ethiopian government has
Related documents