ICF
Scaling Up Chlorhexidine Cord Care for Newborns in Liberia
The Maternal and Child Survival Program (MCSP) collaborated with the Ministry of Health (MOH) in Liberia to improve the delivery of quality maternal, newborn, and child health services.
2018 · 6 pages
Sign in to readA free account is required to download.
Abstract
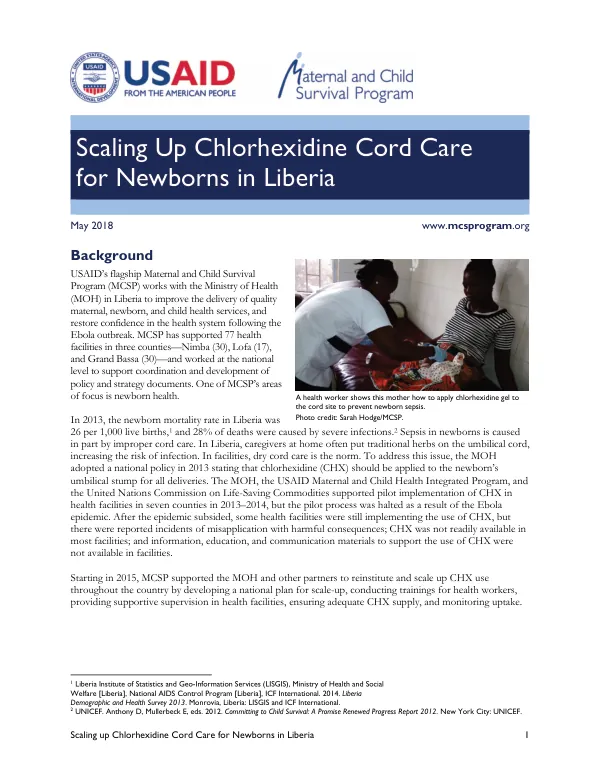
MCSP supported 77 health facilities in three counties—Nimba, Lofa, and Grand Bassa—and worked at the national level to coordinate and develop strategy documents. One of MCSP's areas of focus was newborn health. Newborn mortality in Liberia was 26 per 1,000 live births in 2013, with 28% of deaths caused by severe infections. Sepsis in newborns was often caused by improper cord care. In Liberia, caregivers at home often applied traditional herbs on the umbilical cord, increasing the risk of infection. In facilities, dry cord care was the norm. To address this issue, the MOH adopted a national policy in 2013 stating that chlorhexidine (CHX) should be applied to the umbilical cord for all deliveries. The MOH, the USAID Maternal and Child Health Integrated Program, and the United Nations Commission on Life-Saving Commodities supported pilot implementation of CHX in seven counties in 2013-2014. However, the pilot process was halted due to the Ebola epidemic. After the epidemic subsided, some health facilities were still implementing CHX, but there were reported incidents of misapplication with harmful consequences; CHX was not readily available in most facilities; and information, education, and communication materials to support the use of CHX were not available. Starting in 2015, MCSP supported the MOH and other partners to reinstitute and scale up CHX use throughout the country. MCSP developed a national plan for scale-up, conducted trainings for health workers, provided supportive supervision in health facilities, ensured adequate CHX supply, and monitored progress. The national plan for scale-up included five strategies: strengthening leadership, governance, and coordination for CHX scale-up; ensuring adequately trained and supervised human capacity; ensuring adequate procurement and distribution of CHX gel; promoting appropriate demand for correct application of CHX; and collecting, reporting, and using health information. The MOH's Family Health Division led CHX scale-up at the national level, coordinating partners through the Reproductive Health Technical Committee. Existing county health teams managed scale-up at the county level, with a focal person in each county. At the district and facility levels, specific officers and supervisors were tasked with scale-up, with technical support from the Reproductive Health Technical Committee. UNICEF conducted a 1-day training of trainers for county-level supervisors from 15 counties on CHX cord care in May 2017. MCSP made adaptations to UNICEF's training materials, which were later endorsed by the MOH for use at the county and health facility levels. MCSP also conducted a full-day training on CHX cord care in each of the three supported counties for supervisors from the district health teams, comprehensive emergency obstetric and newborn care health facilities, and other facilities. The training covered refreshers on essential newborn care, evidence on CHX cord care, and methods for counseling caregivers on its use and how to avoid misapplication. Trainers demonstrated CHX application and record-keeping for effective monitoring and evaluation of CHX cord care practices. MCSP supported facility orientation of staff in the 77 health facilities, delivering training sessions through presentations, questions, and answers, and demonstration and practice. MCSP also distributed counseling job aids for health workers and caregivers through collaboration with UNICEF. The national plan strategy for ensuring adequate procurement and distribution of CHX included procuring the first batch of 200,000 tubes of 7.1% CHX in late 2016, sufficient for the first 4 years of the national scale-up. MCSP worked with health facility staff, county health teams, and the MOH to ensure CHX availability in MCSP-supported facilities, providing technical assistance to forecast and submit quarterly requisitions for the product based on their number of deliveries and targets. These requisitions were sent to the counties for compilation and then forwarded to the supply chain unit of the MOH for distribution. By the end of 2018, 75% of all newborns delivered in health facilities were expected to receive CHX. Starting in 2019, CHX was to be expanded to those delivering at home, with the goal of 85% of all newborns receiving CHX by the end of 2021.
Related documents