CAROLINA POPULATION CENTER AT THE UNIVERSITY OF NORTH CAROLINA AT CHAPEL HILL
Strengthening Community Event-Based Surveillance in Senegal
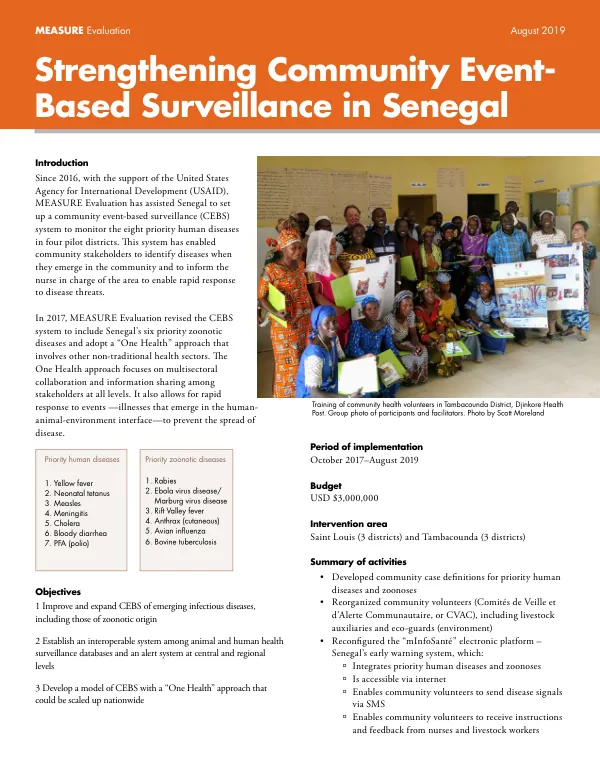
The community event-based surveillance (CEBS) system in Senegal was established in 2016 with the support of the United States Agency for International Development (USAID).
2019 · 2 pages
Sign in to readA free account is required to download.
Abstract
The system aimed to monitor eight priority human diseases in four pilot districts. Community stakeholders were empowered to identify diseases when they emerged in the community and inform the nurse in charge to enable rapid response to disease threats. In 2017, MEASURE Evaluation revised the CEBS system to include Senegal's six priority zoonotic diseases and adopt a "One Health" approach. This approach involves multisectoral collaboration and information sharing among stakeholders at all levels, allowing for rapid response to events that emerge in the human-animal-environment interface. The revised system focused on improving and expanding CEBS of emerging infectious diseases, including those of zoonotic origin. The CEBS system was implemented in two regions: Saint Louis (three districts) and Tambacounda (three districts). The system was developed to integrate priority human diseases and zoonoses, making it accessible via the internet and enabling community volunteers to send disease signals via SMS. The system also enabled community volunteers to receive instructions and feedback from nurses and livestock workers. Community health volunteers were trained in the One Health approach, and multisectoral groups were trained in the CEBS system. A total of 3,377 community volunteers were trained, including 150 nurses, 32 heads of veterinary posts, five private veterinarians, six environmental officers, and 3,377 community volunteers. The system also raised community awareness through schools about the One Health approach and human diseases and zoonoses. During the implementation period (October 2017-August 2019), community volunteers sent 1,650 signals indicating potential disease, with 999 of these cases verified by providers. Of the verified signals, 744 were verified within 48 hours, and 617 were categorized as suspect cases. The CEBS system was successful in reducing delays between the onset of symptoms and the response, and real-time notification of cases by community actors was beneficial. However, challenges were encountered during the implementation of the CEBS system. These included the need to institutionalize the CVAC role and strengthen supervision to motivate community volunteers. Limited logistical support of service providers affected the verification of signals, and there was a need for more livestock providers. Unstable or absent telephone networks in certain areas also posed a challenge for sending and receiving signals. Despite these challenges, the CEBS system in Senegal was successful in improving and expanding CEBS of emerging infectious diseases, including those of zoonotic origin. The system's participatory and inclusive approach allowed for strong ownership at all levels, and organizing diverse groups of community actors was beneficial. The involvement and support of management teams had an important impact on the performance of community stakeholders.
Related documents