WORLD HEALTH ORGANIZATION
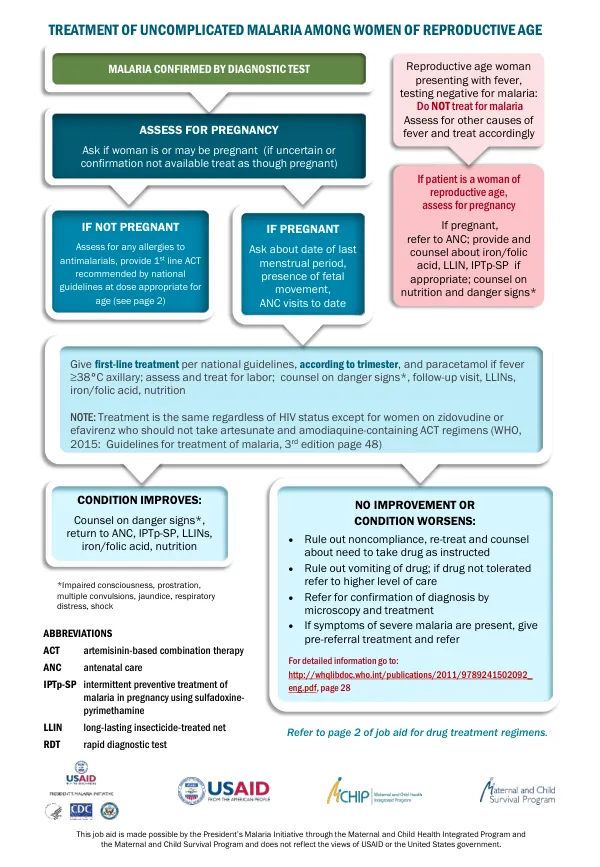
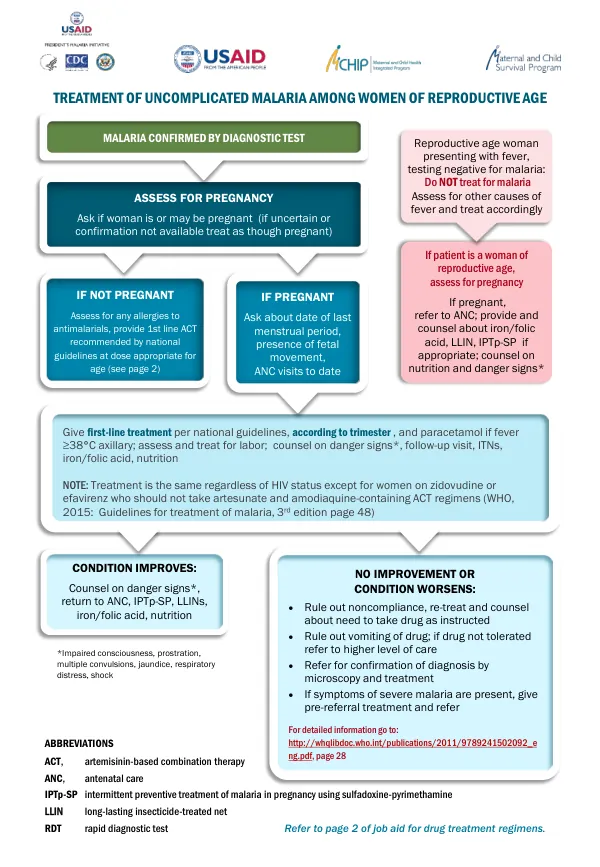
Treatment of Uncomplicated Malaria Among Women of Reproductive Age
Malaria treatment among women of reproductive age is a critical public health concern.
2015 · 2 pages
Sign in to readA free account is required to download.
Abstract
The World Health Organization (WHO) has established guidelines for the management of uncomplicated and severe malaria in this population. Uncomplicated malaria is characterized by the presence of malaria parasites in the blood, accompanied by clinical features such as fever, anemia, and impaired consciousness. Women of reproductive age presenting with fever should be assessed for malaria using a rapid diagnostic test (RDT) or microscopy. If malaria is confirmed, treatment should be initiated promptly. The first-line treatment for uncomplicated malaria in the first trimester is oral quinine salt, administered at a dose of 10 mg/kg every 8 hours for 7 days. Additionally, clindamycin 10 mg/kg orally twice daily for 7 days may be given if available. Artemisinin-based combination therapy (ACT) is indicated only if oral quinine is not available or treatment with quinine plus clindamycin fails. ACTs recommended by WHO, such as artemether/lumefantrine or artesunate/amodiaquine, may also be used as first-line treatment. In the second and third trimesters, ACTs are preferred over oral quinine. The recommended ACTs include artemether/lumefantrine, artesunate/amodiaquine, and other ACTs recommended by WHO. Second-line drugs include artesunate plus clindamycin, ACTs recommended as first-line drugs for the second and third trimesters, and oral quinine plus clindamycin. Severe malaria is a life-threatening condition that requires immediate treatment. Women of reproductive age presenting with severe malaria should be treated with parenteral artesunate as the first-line drug. If artesunate is unavailable, intramuscular artemether or parenteral quinine may be used as second-line drugs. Stabilization and pre-referral treatment for severe malaria include ensuring airway patency, administering oxygen, and treating convulsions and fever. Pregnant women with severe malaria may experience uterine cramping or contractions, which should be managed according to reproductive health guidelines. Hyperparasitemia, defined as parasite densities above 100,000/µL in low transmission areas or 250,000/µL in areas of high stable malaria transmission, is a critical indicator of severe malaria. The management of uncomplicated and severe malaria in women of reproductive age requires careful consideration of the patient's clinical presentation, pregnancy status, and availability of treatment options. Healthcare providers should adhere to WHO guidelines and country-specific recommendations for malaria treatment to ensure optimal outcomes for this vulnerable population.
Related documents