USAID DEC
A Regional Assessment of Facility-Level Maternity and Perinatal Death Surveillance and Response Systems in Four Sub-Saharan Countries
Sign inSAVE THE CHILDREN FUND
A Regional Assessment of Facility-Level Maternity and Perinatal Death Surveillance and Response Systems in Four Sub-Saharan Countries
Maternal and perinatal death surveillance and response (MPDSR) systems are crucial components of strategies to decrease preventable maternal and perinatal deaths in sub-Saharan Africa.
2018 · 1 pages
Sign in to readA free account is required to download.
Abstract
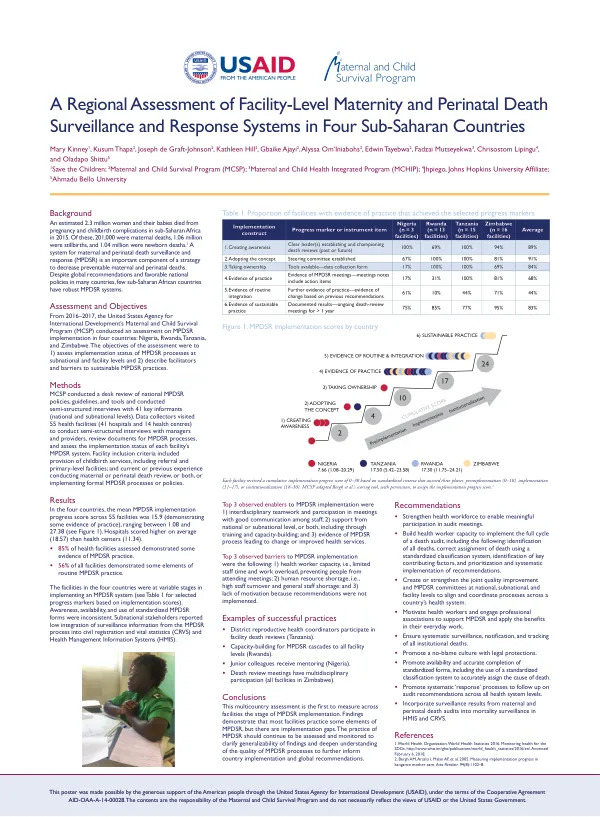
An estimated 2.3 million women and their babies died from pregnancy and childbirth complications in the region in 2015, with 201,000 maternal deaths, 1.06 million stillbirths, and 1.04 million newborn deaths. The United States Agency for International Development's Maternal and Child Survival Program (MCSP) conducted an assessment on MPDSR implementation in four countries: Nigeria, Rwanda, Tanzania, and Zimbabwe, from 2016-2017. The objectives of the assessment were to assess the implementation status of MPDSR processes at subnational and facility levels and to describe facilitators and barriers to sustainable MPDSR practices. The assessment involved a desk review of national MPDSR policies, guidelines, and tools, as well as semi-structured interviews with 41 key informants at national and subnational levels. Data collectors visited 55 health facilities, including 41 hospitals and 14 health centers, to conduct semi-structured interviews with managers and providers, review documents for MPDSR processes, and assess the implementation status of each facility's MPDSR system. The facilities included in the assessment provided childbirth services, including referral and primary-level facilities, and had current or previous experience conducting maternal or perinatal death review or implementing formal MPDSR processes or policies. The results of the assessment showed that the mean MPDSR implementation progress score across 55 facilities was 15.9, with a range of 1.08 to 27.38. Hospitals scored higher on average (18.57) than health centers (11.34). Eighty-five percent of health facilities assessed demonstrated some evidence of MPDSR practice, and 56% of all facilities demonstrated some elements of routine MPDSR practice. The facilities in the four countries were at variable stages in implementing an MPDSR system, with awareness, availability, and use of standardized MPDSR forms being inconsistent. Subnational stakeholders reported low integration of surveillance information from the MPDSR process into civil registration and vital statistics (CRVS) and Health Management Information Systems (HMIS). The top three observed enablers to MPDSR implementation were interdisciplinary teamwork and participation in meetings with good communication among staff, support from national or subnational level, or both, including through training and capacity-building, and evidence of MPDSR process leading to change or improved health services. The top three observed barriers to MPDSR implementation were health worker capacity, including limited staff time and work overload, preventing people from attending meetings, human resource shortage, including high staff turnover and general staff shortage, and lack of motivation because recommendations were not implemented. Examples of successful practices included district reproductive health coordinators participating in facility death reviews in Tanzania, capacity-building for MPDSR cascades to all facility levels in Rwanda, junior colleagues receiving mentoring in Nigeria, and death review meetings having multidisciplinary participation in all facilities in Zimbabwe. The assessment concluded that most facilities practice some elements of MPDSR, but there are implementation gaps. The practice of MPDSR should continue to be assessed and monitored to clarify generalizability of findings and deepen understanding of the quality of MPDSR processes to further inform country implementation and global recommendations. Recommendations included strengthening the health workforce to enable meaningful participation in audit meetings, building health worker capacity to implement the full cycle of a death audit, creating or strengthening joint quality improvement and MPDSR committees at national, subnational, and facility levels, motivating health workers and engaging professional associations to support MPDSR, ensuring systematic surveillance, notification, and tracking of all institutional deaths, promoting a no-blame culture with legal protections, promoting availability and accurate completion of standardized forms, and incorporating surveillance results from maternal and perinatal death audits into mortality surveillance in HMIS and CRVS.
Related documents