SAVE THE CHILDREN FUND
Flow Chart of Specific Management of Postpartum Hemorrhage (PPH)
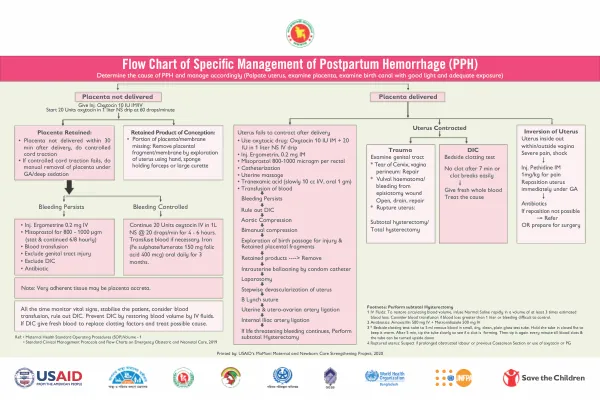
Postpartum Hemorrhage (PPH) Management Flow Chart The management of postpartum hemorrhage (PPH) involves a stepwise approach to determine the cause and implement appropriate interventions.
2020 · 1 pages
Sign in to readA free account is required to download.
Abstract
The first step is to determine the cause of PPH and manage accordingly. This includes palpating the uterus, examining the placenta, and examining the birth canal with good light and adequate exposure. If the placenta is not delivered, the recommended interventions include administering intramuscular (IM) or intravenous (IV) oxytocin 10 IU, starting a 20-unit oxytocin infusion in 1 liter of normal saline (NS) at 60 drops per minute, and performing controlled cord traction. If controlled cord traction fails, manual removal of the placenta under general anesthesia (GA) or deep sedation is recommended. If bleeding persists, additional interventions include administering ergometrine 0.2 mg IV, misoprostol 800-1000 micrograms, and blood transfusion. It is also essential to exclude genital tract injury and disseminated intravascular coagulation (DIC). Antibiotics may also be administered to prevent infection. Retained products of conception, including portions of the placenta or membranes, require removal by exploration of the uterus using a hand, sponge-holding forceps, or a large curette. If bleeding is controlled, the recommended interventions include continuing the oxytocin infusion for 4-6 hours, transfusing blood if necessary, and administering iron supplements for 3 months. In cases where the uterus fails to contract after delivery, oxytocic drugs such as oxytocin, ergometrine, and misoprostol may be administered. Uterine massage, catheterization, and tranexamic acid may also be used to stimulate uterine contractions. If bleeding persists, further interventions include ruling out DIC, performing aortic compression, and exploring the birth passage for injury and retained placental fragments. In severe cases of PPH, more invasive interventions may be necessary, including intrauterine ballooning by condom catheter, laparotomy, stepwise devascularization of the uterus, B-Lynch suture, utero-ovarian artery ligation, and internal iliac artery ligation. If life-threatening bleeding continues, subtotal hysterectomy may be performed. In cases of trauma, DIC, or rupture of the uterus, additional interventions may be necessary, including examining the genital tract, performing bedside clotting tests, and repairing any tears or lacerations. In cases of inversion of the uterus, immediate repositioning under GA may be necessary, and antibiotics may be administered to prevent infection. Overall, the management of PPH requires a comprehensive approach that involves determining the cause, implementing appropriate interventions, and monitoring vital signs to prevent complications.
Related documents