USAID DEC
Bridging the Gap in Ebola Prevention and Response in Côte d'Ivoire’s At-Risk Border Region
Sign inINTERNATIONAL FEDERATION OF THE RED CROSS AND THE RED CRESCENT SOCIETIES
Bridging the Gap in Ebola Prevention and Response in Côte d'Ivoire’s At-Risk Border Region
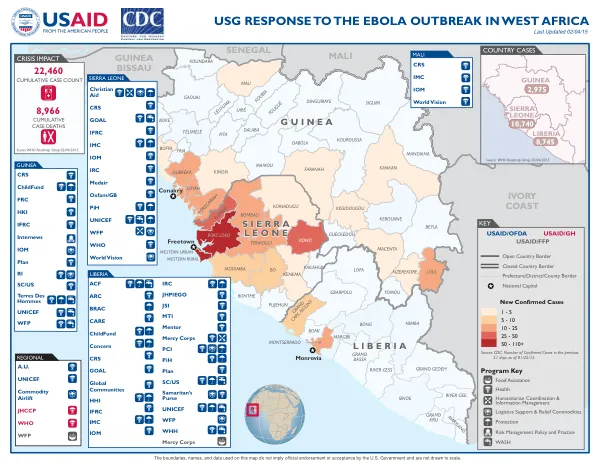
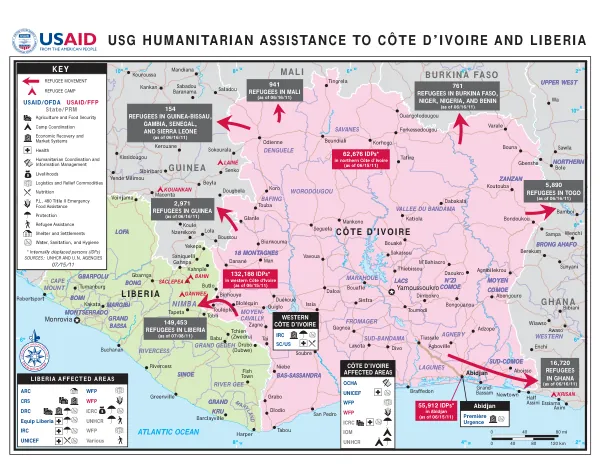
The Ebola outbreak, declared in Guinea in March 2014, quickly spread to neighboring countries, namely Liberia and Sierra Leone.
2015 · 15 pages
Sign in to readA free account is required to download.
Abstract
The epidemic is the deadliest since the first cases were reported in 1976 in Democratic Republic of Congo. As of November 4, 2015, there were 28,571 reported cases of Ebola virus disease (EVD) in Guinea, Liberia, and Sierra Leone, with 11,299 reported deaths. The risk of importing an EVD case remains a very real threat to Côte d'Ivoire due to its proximity with Guinea, porous borders, and cross-border social and commercial activities. The Government of Côte d'Ivoire, particularly its Ministry of Health (MoH), took its first preventive measures in March 2014, followed in September 2014 by a National Plan on Ebola Fever Prevention and Response to address the worsening situation in neighboring countries. The national plan focuses on six key objectives: planning and coordination of the response, communication and sensitization, epidemiological surveillance, prevention measures, health system response capacities, and research. The government of Côte d'Ivoire sought the support of technical and financial partners, such as the International Rescue Committee (IRC), to strengthen its response to the Ebola outbreak. The IRC Côte d'Ivoire's health team has been implementing Ebola prevention and response activities since April 2014 in 137 health facilities along the Western border with Liberia and Guinea. In November 2014, the IRC carried out a rapid needs assessment in the Northern districts of Touba, Odienné, and Minignan (Kabadougou-Bafing-Folon health region). The assessment showed that the level of preparedness to respond to potential Ebola cases was very low in those three districts. The IRC found that coordination, surveillance, prevention, and response mechanisms required urgent strengthening in order to be functional. Based on these observations, USAID provided generous support to the IRC to expand the intervention to the rest of the sensitive border area. The USAID-funded project began on December 19, 2014, and ended on August 18, 2015. The IRC supported activities that focused on community sensitization, training and equipping of community members and health facility staff to adequately respond to a potential outbreak, improving the early detection and epidemic surveillance system in supporting vulnerable health regions along the Liberia and Guinea borders. The IRC contributed to Ebola prevention and response activities in the targeted areas through close collaboration with decentralized health authorities and by following the National Plan on Ebola Fever Prevention and Response. The IRC worked with key stakeholders at all levels to carry out these activities, including those at central, regional, and district levels, as well as international and local NGOs and UN Agencies. The IRC systematically coordinated the intervention with partnering health facilities and regional and district management teams. The IRC started the recruitment of project staff in early January 2015. This process took about six weeks and was finalized by mid-February 2015. The IRC worked closely with local administrative authorities, including prefects and sub-prefects, who led coordination activities in each district. The IRC also participated in monthly meetings in Abidjan and in the field with national institutions, other humanitarian actors, UN agencies, and bilateral donors to look for synergies and avoid duplication. The IRC's health team conducted two exploratory missions in the districts of Touba, Odienné, and Minignan in November and December 2014. As a result of these missions, the team confirmed the existence of significant gaps in the districts' preparedness as compared with other districts along the same border receiving support from other international NGOs and national authorities. The IRC deemed additional practical trainings, protective equipment, and effective epidemiological surveillance and response mechanisms to be urgently needed. The IRC implemented various program activities, including community sensitization, training and equipping of community members and health facility staff, improving the early detection and epidemic surveillance system, and strengthening regional-level capacities for responding to Ebola. The IRC worked closely with local administrative authorities, health facilities, and regional and district management teams to implement these activities. The IRC also participated in monthly meetings with national institutions, other humanitarian actors, UN agencies, and bilateral donors to look for synergies and avoid duplication. The IRC's program activities focused on five objectives: coordination, sensitization, epidemiological surveillance, prevention, and response. The IRC worked with key stakeholders at all levels to carry out these activities, including those at central, regional, and district levels, as well as international and local NGOs and UN Agencies. The IRC systematically coordinated the intervention with partnering health facilities and regional and district management teams. The IRC's program activities resulted in improved regional-level Ebola planning and coordination, increased community awareness of the risks and transmission mechanisms of the Ebola virus, strengthened epidemiological surveillance, improved Ebola transmission prevention measures, and strengthened regional-level capacities for responding to Ebola. The IRC's program activities also resulted in improved communication, visibility, and information activities, as well as lessons learned and constraints identified during the implementation of the program.
Related documents