USAID DEC
Can depression treatment feasibly be integrated into high-volume, routine HIV care in Malawi?
Sign inMINISTRY OF HEALTH
Can depression treatment feasibly be integrated into high-volume, routine HIV care in Malawi?
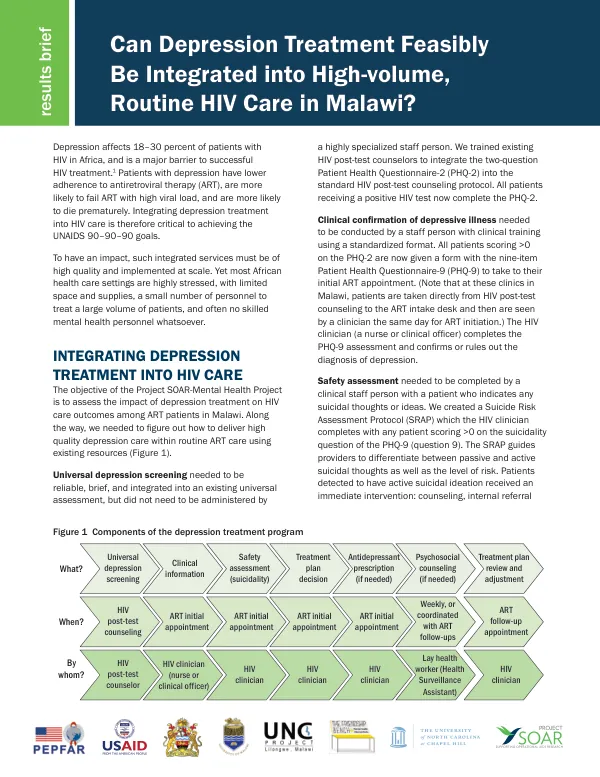
Depression affects 18-30 percent of patients with HIV in Africa, and is a major barrier to successful HIV treatment.
2021 · 4 pages
Sign in to readA free account is required to download.
Abstract
Patients with depression have lower adherence to antiretroviral therapy (ART), are more likely to fail ART with high viral load, and are more likely to die prematurely. Integrating depression treatment into HIV care is therefore critical to achieving the UNAIDS 90-90-90 goals. The Project SOAR-Mental Health Project aimed to assess the impact of depression treatment on HIV care outcomes among ART patients in Malawi. The project focused on delivering high-quality depression care within routine ART care using existing resources. Universal depression screening was integrated into the existing universal assessment, and patients scoring >0 on the Patient Health Questionnaire-2 (PHQ-2) were given a form with the nine-item Patient Health Questionnaire-9 (PHQ-9) to take to their initial ART appointment. Clinical confirmation of depressive illness was conducted by a staff person with clinical training using a standardized format. Safety assessment was completed by a clinical staff person with a patient who indicated any suicidal thoughts or ideas. A Suicide Risk Assessment Protocol (SRAP) was created to guide providers to differentiate between passive and active suicidal thoughts as well as the level of risk. Patients detected to have active suicidal ideation received an immediate intervention: counseling, internal referral to the clinic's mental health team, or external referral to the district secondary tier mental health clinic, depending on severity of the suicidal ideation and resources at the clinic. The depression treatment plan was determined by the HIV clinician, guided by a treatment algorithm. HIV clinicians were trained to prescribe antidepressants when indicated, and Health Surveillance Assistants (HSAs) were trained to provide psychosocial counseling using the Friendship Bench problem-solving therapy protocol. The depression treatment plan was reviewed and adjusted, if needed, based on the algorithm by the HIV clinicians at routine ART follow-up appointments. Fidelity in delivering antidepressant treatment was high, with providers achieving high fidelity in starting a patient on an antidepressant when indicated and at the recommended dose. However, fidelity was more limited in re-administering the PHQ-9 at follow-up visits for patients started on an antidepressant. Among follow-up visits for patients currently on an antidepressant, only about two-thirds remained on that antidepressant; the remainder discontinued or switched medication. Generally, depressive symptoms and suicidal thoughts have decreased markedly in patients starting treatment. Among patients starting an antidepressant, the median PHQ-9 score decreased from 11 at ART treatment initiation to 3.5, 3, and 0 at the first, second, and third month in care, respectively. The proportion of patients with any report of suicidal thoughts decreased from 39 percent at baseline to between 10 and 24 percent at follow-up visits. Among patients starting the Friendship Bench counseling program, who had PHQ-9 scores of 5-9 at baseline, the median PHQ-9 score decreased from 6 at ART treatment initiation to 1, 0, and 0 at the first, second, and third month in care, respectively. The proportion of patients with any report of suicidal thoughts decreased from 14 percent at baseline to between 4 and 7 percent at follow-up visits.
Related documents