GOVERNMENT OF INDONESIA
Improving Maternal Health Services in India: A Compilation of Change Ideas
The maternal health services in India underwent significant improvements during the antenatal period.
2015 · 4 pages
Sign in to readA free account is required to download.
Abstract
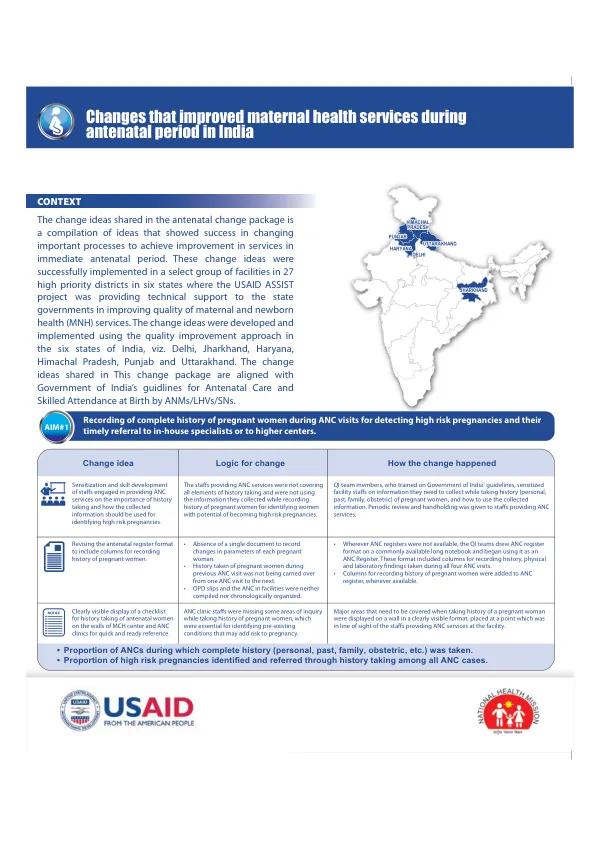
A key change idea involved sensitizing staff engaged in providing antenatal care (ANC) services on the importance of history taking and how the collected information should be used for identifying high-risk pregnancies. Initially, staff were not covering all elements of history taking and were not using the information they collected while recording the history of pregnant women for identifying women with potential high-risk pregnancies. Quality improvement (QI) team members, who were trained on Government of India guidelines, sensitized facility staff on the information they needed to collect while taking history (personal, past, family, obstetric) of pregnant women, and how to use the collected information. Periodic review and handholding were given to staff providing ANC services. To facilitate this, the antenatal register format was revised to include columns for recording history of pregnant women. A clearly visible display of a checklist for history taking of antenatal women was placed on the walls of MCH centers and ANC clinics for quick and ready reference. This ensured that ANC clinic staff were missing fewer areas of inquiry while taking history of pregnant women, which was essential for identifying pre-existing conditions that may add risk to pregnancy. The proportion of ANCs during which complete history (personal, past, family, obstetric, etc.) was taken increased, and the proportion of high-risk pregnancies identified and referred through history taking among all ANC cases also improved. Another change idea involved measuring and recording hemoglobin (Hb) levels in all antenatal check-ups and their timely referral to in-house specialists or to higher facilities. Initially, Hb testing was being done for all pregnant women on their first ANC visit, but subsequent Hb testing was not consistent across different facilities. The QI teams sensitized facility staff on the importance of Hb testing during every antenatal visit and on how to use changes detected in Hb levels in identifying high-risk pregnancies and managing them. A separate column was added to the ANC register for recording Hb levels for all four ANC visits. Staff nurses were instructed to record Hb levels for all ANC patients in that column, and all staff providing ANC services were oriented to mark cases where Hb level is less than 11 gm/dL in the ANC register as high risk for further action (management or referral). In addition, orientation and training were provided to all paramedical staff on the importance of measuring and recording blood pressure (BP) for women during every antenatal check-up and the correct way to measure BP. Initially, health facility staff did not understand the value of measuring BP in every ANC visit to identify high-risk pregnancies, and in some cases, they were also incorrectly measuring BP. Medical officers in-charge (MOIC) trained all healthcare staff of the facility on the importance of measuring and recording BP in all ANC visits of a pregnant woman. The health staff were given hands-on training in measuring BP, and a new column was added to the ANC register to record BP of pregnant women for all ANC visits. Staff were oriented to identify pregnant women whose BP level was more than 140/90 and mark them in the ANC register as high risk for further action (management or referral). Furthermore, the out-patient department (OPD) hours were redistributed to make time for a separate timeslot dedicated only to ANC services. Pregnant women coming to the health facility were not getting all ANC services due to high patient load and clash of timing of ANC and immunization services. The MOIC of the facility scheduled immunization services from 8 AM to 11 AM daily and ANC services from 11 AM to 2 PM in the OPD for all days, which freed up time of the nursing staff to measure blood pressure of all pregnant women. The ANC room was also relocated to the ground floor and adjacent to the female outpatient department (OPD) in the health facility. Initially, the female OPD was on one floor while the ANC room was on a different floor, resulting in pregnant women going home after consulting the medical officer in the female OPD without getting their vitals checked with staff in the ANC room. Finally, clarifying roles and task shifting of measuring BP involved assigning staff for checking and recording BP of pregnant women, enabling ASHAs to measure BP using digital BP apparatus, and ensuring that no service was missed to a pregnant woman during the antenatal visit through regular review of records and patient interviews. The MOIC of the facility trained the identified ASHAs during their monthly meeting on measuring blood pressure using the digital BP machine, and a senior staff was made responsible to ensure that no service was missed to a pregnant woman during the antenatal visit. In-house maintenance of consolidated ANC records of pregnant women coming to the facility for ANC services for tracking and managing high-risk pregnancies was also implemented. Initially, clinical details were being recorded on a new antenatal card every time a pregnant woman went to a different facility for ANC visit, resulting in ANC information not getting consolidated. The USAID ASSIST Project acknowledges the unw